UserWiki:Richardpruen: Difference between revisions
Richardpruen (talk | contribs) Add Letter sec state health and social care 14 March 2024 |
Richardpruen (talk | contribs) add letter to DHSC 13 april |
||
| (17 intermediate revisions by the same user not shown) | |||
| Line 30: | Line 30: | ||
Twitter [http://twitter.com/pruenrichard @pruenrichard] | Twitter [http://twitter.com/pruenrichard @pruenrichard] | ||
Below are letters and documents sent in advocacy efforts as a record and should anyone wish to use them for ideas. These are my efforts and do not necessarily reflect the views of the wiki or other users. | |||
[[File:FDA comment.pdf|thumb|alt=Comment on R-U FDA review |Comment on R-U FDA review ]] | [[File:FDA comment.pdf|thumb|alt=Comment on R-U FDA review |Comment on R-U FDA review ]] | ||
| Line 60: | Line 62: | ||
[[File:Letter sec state health and social care 14 March 2024.pdf|thumb|alt=Subject: Youth vaping Please see the above graph, so far regular use (greater than once a week) is not high and may be displacing cigarettes, cigarettes are the worlds most deadly consumer product. Infrequent and trial use (once in 30 days, or ever use) while undesirable does not lead to dependence, only those in the graph above can possibly be ‘hooked’, but not all will be. I do not think young people should be encouraged to vape, but I would like to know your answer to one question, please. If a young person is determined to use nicotine, would you advise them to smoke cigarettes instead of safer alternatives, and a what age should harm reduction products like vaping be made available. I look forward to receiving your answer. Please feel free to ask others what they think should be done. Personally I feel the situation in Sweden is close to the best balance, accepting some use of low risk Snus, in order to reduce the uptake of deadly smoking. This will take effect far faster than the generational tobacco ban, Sweden will be a non smoking nation this year, although nicotine use remains, they have the lowest cancer rate in Europe. The UK can easily and quickly achieve the same with vaping. I note also Sweden reduced the tax on Snus to accelerate uptake. Yours sincerely, Richard Pruen|Letter sec state health and social care 14 March 2024]] | [[File:Letter sec state health and social care 14 March 2024.pdf|thumb|alt=Subject: Youth vaping Please see the above graph, so far regular use (greater than once a week) is not high and may be displacing cigarettes, cigarettes are the worlds most deadly consumer product. Infrequent and trial use (once in 30 days, or ever use) while undesirable does not lead to dependence, only those in the graph above can possibly be ‘hooked’, but not all will be. I do not think young people should be encouraged to vape, but I would like to know your answer to one question, please. If a young person is determined to use nicotine, would you advise them to smoke cigarettes instead of safer alternatives, and a what age should harm reduction products like vaping be made available. I look forward to receiving your answer. Please feel free to ask others what they think should be done. Personally I feel the situation in Sweden is close to the best balance, accepting some use of low risk Snus, in order to reduce the uptake of deadly smoking. This will take effect far faster than the generational tobacco ban, Sweden will be a non smoking nation this year, although nicotine use remains, they have the lowest cancer rate in Europe. The UK can easily and quickly achieve the same with vaping. I note also Sweden reduced the tax on Snus to accelerate uptake. Yours sincerely, Richard Pruen|Letter sec state health and social care 14 March 2024]] | ||
[[File:Letter sec state health and social care 11 May 2024.pdf|thumb|alt=Subject: Tobacco and vapes bill Dear Victoria Atkins, I am contacting you as a vaping consumer, and advocate for saving lives, vaping saved my life (happy to share medical records to prove that) and I aim to pass that on to as many as possible, I am not paid in any way by anyone to do so. I was disturbed to hear some of the testimony given in parliament, much of the information was incorrect, or deliberately misleading. This is not good enough when debating a serious matter of health, accurate and science backed information is critical to saving lives. I would like an answer to the following question: What was the reason to justify excluding stakeholders, the users of vaping products, other safer tobacco products, and even people who smoke? User funded charities such as New Nicotine Alliance, who take no money from the tobacco or vaping industry should have been consulted. Users themselves or NNA would have been able to counter some of the poor information given and also to provide a view from those directly affected by the legislation being discussed. Much of the information could have been corrected, quickly and easily. The main issues with the unopposed debate (no stakeholder representative, or consideration given to stakeholders, it seems); the conflation of illegal/criminal imports of untested and illegal drug products, and legal UK nicotine vaping; the lack of separation between the independent vaping industry and tobacco multinationals (they are not the same thing); the potential to harm the UK government stop to swap scheme (saving lives of people who smoke now, not a future population, years from now)… I could go on, but others like UK Vaping Industry Association have pointed out the issues, no need for a repeat. My most important question; What is being done to ensure that stakeholders are heard, and the users of these products are not swept aside? Particularly what is being done to ensure false/misleading statements are not made to parliament by the experts, or that at least someone is included on behalf of users to set the record straight? I look forward to your responses. Yours sincerely, Richard Pruen|Letter sec state health and social care 11 May 2024]] | |||
[[File:Draft redact address letter PM 8th Jul 2024.pdf|thumb|alt=Subject: The ban on disposable cigarettes / vaping in general | |||
Dear Prime Minister, | |||
I am a consumer advocate for vaping (15 years and a vaper for 16), and I do not use disposables beyond experimenting to see what they are like. I am also an engineer. I have previously worked in the vaping industry, testing against the standards for vaping products, and owned a now-closed company, BTC Battery Testing LTD (closed 2016). I am a consumer now and take no money from any industry, charity, or government scheme. Currently, I care for my mother, who suffers from vascular dementia, and as such, I volunteer my spare time to the cause of THR. I also advocate for smoking cessation in sufferers of severe mental health conditions. ASH UK funds the group, but I do not take any payment for my time. Regarding the subject. Might I remind you that Australia has already taken this path? An effective ban, over 80 fire bombings, at least three gang-style murders, and a rampant illegal trade have resulted? It simply won’t work. The prohibitionist faction has played on children starting using these products, and may have convinced you that a ban is enforceable; sadly, if Australia cannot do it, the proximity of Europe means less chance here. I am simply being realistic. The best, perhaps only, way to control the illicit trade is to make sure there is a legal trade that makes it less profitable; the US abandoned alcohol prohibition in favour of this. Please, however, remain focused on preventing harm; having the only source of disposable vapes (sorry to say this, but it is true) that adolescents could buy, being from a ‘dealer’ who might supply other illicit substances, is not safer! At least if they are from a shop selling tested, safe devices, then that is a vast reduction in harm already, avoiding interaction with drug dealers. I prefer every shop to follow the law, but as we know, not everyone will. Adolescents might also sample smoking, especially if they sensibly avoid illicit substance dealers; this, too, is not exactly a win, smoking being deadly and carcinogenic. Those diverted from cigarettes face a much lower risk of cancer and other smoking-related diseases. It is a fact that zero deaths have been caused by vaping a regulated nicotine product; among around 82 million users worldwide, the EVALI deaths all resulted from an illegal trade in THC vaping in the US (different chemistry and devices, incompatible with nicotine vapes). I favour regulations to encourage the use of rechargeable vapes. However, even disposables can be recycled; these are far superior to cigarette filters; filter tips are nearly impossible to recycle and will be in the environment for years. Exceptions should be made for disabled people (unable to fill or use pods) in secure mental health care/prisons; here, disposable tamper-resistant devices are safer. However, legislation should favour the refillable and reusable vapes that are most environmentally sound; disposables can be discouraged without a ban. Please see the graph. So far, regular use is not high and may be displacing cigarettes. Sensible regulations to keep it that way would be welcome. A few truths to bear in mind: The use of the word ‘children’ is a deliberate tactic to tug on heart strings, more correctly teens particularly adolescents are at risk from experimenting with vapes and other adult things, harm reduction still applies, beer is safer than vodka, vapes are vastly safer than cigarettes. Infrequent trial use isn’t the best indicator of dependence (once in 30 days), better is once a week or more. To risk dependence you need to be regularly vaping. The harm from vaping is low enough it is right to argue against the use of addiction, since the DSM-5 definition requires significant harm, dependence is more correct because it can be hard to stop. Vaping allows users to taper nicotine so less than cigarettes. Millions of lives are at stake, billions of pounds the NHS spend on cancer and other smoking related treatments that could be eliminated, smoking is the leading cause of preventable death, vaping regulated nicotine products, zero deaths in 20 years. The less popular you make vaping, the more popular smoking will become, they are substitutes. When you ban things; illicit markets form, they have no reason to follow age of sale or other rules, this risks making things worse not better (Australia demonstrates this). The generational ban while it sounds good, kicks the can into the future, vaping is reducing smoking right now, and more effort is required to target older adults, they are the ones facing smoking related diseases imminently, switching them to vapes is a huge immediate benefit the generational ban could never deliver. I would like to hear your thoughts, I will be happy to provide evidence to support what I have said, if required for any point please let me know. You promised your government would work for us, and would look after our health and well-being, here is a way to prove you will listen, many lives can be saved. If there is one single study I think most important: Comparison of biomarkers of exposure among US adult smokers, users of electronic nicotine delivery systems, dual users and nonusers, 2018–2019. For every harmful or potentially harmful compound, vapers look exactly like non-users. Thank you for your time, I have tried to be brief as you must be busy, but welcome questions should you have any. Yours sincerely, Richard Pruen P.S. My story: Why I do this? I started vaping in 2008 when it was relatively new, I had at this point given up trying to stop smoking, having tried everything. I intended to vape where I was unable to smoke. To my surprise in March of 2009 I discovered I had money budgeted for cigarettes that was unspent, this was how I discovered I had accidentally given up smoking. In 2010 I watched my father die from cancer, smoking 20/day didn’t help, although as a firefighter there is occupational risk also. My health improved substantially over the first 5 years, and at 15 years vaping I had an MRI due to aortic aneurysms running in the family (my father had one repaired), my lungs where those of a non smoker, doctors where unable to find any sign I vape. Put simply vaping saved my life and I would like pass that forward, partly in memory of my father, he was a firefighter and lived to save lives. |draft letter to new PM for 8th JUL]] | |||
[[File:Draft redact address letter wes sweeting 15th Jul 2024.pdf|thumb|alt=Subject: Tobacco and vapes bill | |||
Dear Wes Sweeting, | |||
I am contacting you as a vaping consumer and advocate for saving lives; vaping saved my life (I am happy to share medical records to prove that), and I aim to pass that on to as many as possible. I am not paid in any way by anyone to do so. I have worked in the vaping industry, helping to develop standards and testing against them (I ran BTC battery testing until 2016). This was good for consumer safety, but the industry did not necessarily favour it. I am also part of a group funded by ASH advocating for smoking cessation in people living with severe mental illness; 40% smoke cigarettes, double the national number. | |||
I was disturbed to hear some of the testimony given in parliament, mainly by the previous government. Much of the information was incorrect or deliberately misleading. You must do better when debating a serious health matter; accurate and science-backed information is critical to saving lives. You should be using the research OHID paid for using taxpayers' money, not anecdotal (often second-hand) accounts from teaching staff or parents frightened by the media (more on that below). | |||
Before proceeding with further legislation, you must pause and ensure stakeholders (particularly end users) are appropriately consulted. Without accurate and proper information, bad legislation will result, like Australia and the prescription model (now dropped, and pharmacy only, also likely to fail) Will Australia's tightened prescription system reduce nicotine vaping among young people? wiley.com and others show the policy failed, and instead 90% supply was from illegal sales controlled by organised crime. At the time of writing this, there have been more than 80 fire-bombings, three murders, and many gang ‘turf-wars’ in Australia. We do not need to bring that here. | |||
Sadly, there is a lot of misinformation being pushed in the media regarding children using these products; the use of ‘children’ is deceptive, even using the over-wide definitions that are often cited; children are not the population at risk. Sales are already illegal to those under 18; advertising to such age groups is also banned, and advertising is generally restricted. Please see my letter to the PM available from my wiki user page (direct link) https://safernicotine.wiki/mediawiki/index.php/File:Draft_redact_address_letter_PM_8th_Jul_2024.pdf. Adolescents are the population who might take up vaping, they might also take up smoking (far more deadly), or experiment with other adult things. It is a part of growing up, and if you prevent the less harmful options, adolescents will probably do more risky things. | |||
I agree that you should keep a close eye on frequent vaping among adolescents; thankfully, that remains low and does not show worrying trends (please see the graph in the letter to PM above). Experimentation with vaping is preferable to cigarettes, and still, too many are starting to smoke tobacco. Vaping is unlikely to cause deaths, at least, unlike tobacco, and has (with open devices) the off-ramp of tapering nicotine slowly (around a third of folks quitting smoking with vapes also stop vaping this way; see ONS data). | |||
It is essential to accept the vastly lower risk when considering legislation that will steer adolescents in a particular direction. Assuming they will do extra homework if they can’t experiment is faulty. They will likely do something more risky instead, such as alcohol. Alcohol, for example, results in accidents, intoxication and deaths. This is sadly human nature, and harm reduction at least keeps the risks as low as possible. | |||
It is also vital to ensure that illicit vapes and illegal sales are kept to a minimum; buying vapes from ‘dealers’ opens all manner of unwanted possibilities, including other more harmful illegal drugs being offered. Thus, great care is needed to avoid a ban on a product type resulting in supply shifting to criminal-controlled illicit sales. There is already too much of this with over-strength/over-capacity disposable vapes; outright bans on disposables will make this far worse. This will require some subtlety and care in regulations to address the issue. Instead of a ban, having the price include the cost of disassembly recovery and recycling might better direct sales to refillable and, thus, much more environmentally friendly devices. The extra complexity of using a pod device is slight, so a small nudge is likely required for most consumers to shift to a more environmentally responsible product. You need to consider things carefully before doing anything and look at the unintended consequences that might occur. | |||
In only five years, New Zealand halved its smoking rate (now approaching 5%). https://www.scoop.co.nz/stories/WO2407/S00138/caphra-calls-on-asia-pacific-governments-to-allow-sale-of-oral-nicotine-products.htm The government there promoted vaping more than the UK government. For comparison, Canada taxes and does not promote vaping, and the smoking rate has remained stable. Sweden recently reduced the tax on Snus in a bid to increase switching (they are about to drop below 5% also) and has had great success with a THR product in Snus. | |||
In Sweden, the use of nicotine is about the same as in the EU as a whole, but the rates of cancer are lower, particularly in men, since they switched earlier, and the trend is now apparent in the data. It is worth looking at Sweden because it has had a harm-reduction product for a long time, and trends and population data are readily available. It is obvious that nicotine is not a problem; it is combusted tobacco, particularly cigarettes; switching existing users to safer products is the priority; you can save vast numbers of lives and treatment costs. I suggest you research the history of THR in Sweden, allowing users to initiate nicotine use with a safer product works; they have the lowest cancer rates in the EU by a good margin. | |||
It is essential to be honest when looking at nicotine; it has benefits for some people; for ADHD, it is an effective treatment. I can help with other things, schizophrenia and depression. There is a list of peer-reviewed science here: https://safernicotine.wiki/mediawiki/index.php/Nicotine_therapeutic_benefits. Not to mention that every military in the world included nicotine in rations and snuff for submariners (since smoking was not possible due to hydrogen from batteries); they would not have gone to such expense if it was not beneficial to highly stressed young soldiers. These reasons mean that some people will use nicotine, so safer options are a win. Nicotine cannot be eradicated as some would wish. Trying to do so will result in uncontrolled illegal sales and crime (please see Australia if you have any doubts). To do the right thing and reduce harm as far as possible, you must look at all this and do your best. There is no clear path; there are always unintended consequences (thankfully, safer nicotine products are very non-deadly compared to cigarettes, so the remaining risk equates to being dependent (this happens with caffeine/coffee/energy drinks with little fuss)). So you have a chance to do what is right by the people you work for, and the NHS, even if it doesn’t fit entirely with popular opinion (partly due to worldwide campaigns by Mike Bloomberg and associated NGOs, they were caught trying to influence government https://mb.com.ph/2021/08/30/local-anti-vaping-groups-also-received-millions-of-grant-money-from-bloomberg/ Bloomberg has also stated “I don’t care if vapes are safer. I want them shut down no matter what” Public health heavyweights and scientists alike have offered to present evidence proving the good from vaping/THR, but have been ignored (repeatedly), Bloomberg’s view seems based not on data, but ideology. | |||
Needless to say, the tobacco and vapes bill is generational prohibition; by the modelling done, it will not do anything until it restricts sales (2040 before results are seen); it risks creating an illegal market and other prohibition-related problems; we can look to Australia to see the sorts of things to expect. Getting vapes out to older adult cigarette users will give results from day one; as soon as someone switches to vaping, the risk of cancer and disease begins to fall. That relieves pressure for treatment from the NHS, which can only be good. | |||
As I see it, you need to stop and take a hard look at the sin tax (it will put folks off switching and give the impression vapes are as bad as smoking) and the tobacco and vapes bill, then it shouldn’t be challenging to find something better. I think vapes should remain tax-free to encourage switching. However, users might put up with a small amount to improve enforcement of underage sales and illegal vapes. (Though there are things that can be done to reduce the waste from disposables by a factor of 10) some ideas in this letter https://safernicotine.wiki/mediawiki/index.php/File:Email_to_appg_vaping_28th_Feb_2023.pdf | |||
One last point, the UN considers harm reduction for drug users to be a human right, and nicotine is a drug. This means that because harm reduction options exist, all with vastly lower risk than cigarettes, you must try to make them available to those at risk from the more harmful combusted tobacco. | |||
Please feel free to ask questions. I will always try to help if possible. Likewise, if you require evidence to support anything I have said, please ask. Alternatively, you can verify with your own research if you wish. Yours sincerely,Richard Pruen|Draft letter Wes Sweeting]] | |||
[[File:Email 6th sept DHSC reply.pdf|thumb|alt=Sirs, Please find my reply inline in answer to your comments below. It is rather long, but a great deal of misinformation needs correcting. On Fri, 2024-09-06 at 10:51 +0000, Department of Health and Social Care wrote: Our ref: DE-1524319 Dear Mr Pruen, Thank you for your correspondence of 5 August about vaping. I have been asked to reply. I appreciate your concerns. The Government recognises the role that vapes can play as a smoking quit aid and it is not its intention to restrict the accessibility of vapes to adults in the upcoming Bill. Any measures brought forward through the upcoming Bill will be designed to curb youth vaping whilst having a minimal impact on adult vapers. The number of children vaping has tripled in the last three years, with one in five having used a vape in 2023, and the Government’s aim is to stop future generations from becoming hooked on nicotine. Regarding the number vaping, very small number tripled is a very small number, for comparison please see the following graph (30 day use for various places) this includes a lot of experimental use that does not lead to dependence, and is sadly a part of growing up, adolescents try adult things (including alcohol at higher rates than vaping, causing deaths). Vaping won't cause any deaths at least, unlike cigarettes (few but fires do happen). As can be seen the rates of infrequent use are the lowest in the UK, and highest in Australia (excluding the blip in the USA). I do not believe this is a coincidence, it reflects the regulation and illegal sales, the UK and Australia being at opposite extremes. Here in the UK vaping is regulated and most sales are legal, from shops that have every reason to restrict sales to adolescents. In Australia the product is illegal without prescription, and 92% of the supply is via illegal sales, leading to firebombings and gang warfare. Illegal sales have every incentive to break the law, and sell to anyone with the cash. Illegal products are entirely unregulated. We need to remain in control of sales, since it is working, the UK has the lowest use among adolescents. Changes risk sending more sales to the illegal market, and reducing control over sales. This will have the opposite effect to the one you intend and result in more sales being illegal and thus more sales to underage. More enforcement of the existing rules, and work to reduce illegal sales would be welcome, and I suggest more useful than further restrictions in remaining in control. Absolutely do not follow Australia, that method/type of control is proven a failure. In the data above from ASH, we can see that 0.8% young people are vaping regularly having not also been a smoker, vaping is vastly safer than smoking, diverting them from cigarettes is a highly positive outcome. Given the data, and we must rely on data and facts here, all but 0.8% are diverted from cigarettes, and that means virtually no smoking naive youth are going on to regularly vape. This quite near to the ideal situation, changes in legislation that might make this worse (by increasing illegal sales) should be avoided. If it is working, don't fix it? While it is certainly true that adults prefer fruit and sweet flavours, many flavours on the market are overly appealing to children.Evidence shows that children are attracted to the fruit and sweet flavours of vapes, both in their taste and smell, as well as how they are described. Many flavours have attractive wording and names that entice children to try vaping, such as ‘gummy bear’ and ‘rainbow burst’. Nonsense, gummy bears are a sweet from my childhood, they may exist still, but I would buy that, I contest that is targeted at memories of adults. You might have more information on this, you should speak to the actual consumers of the product before jumping to easy sounding conclusions. New Nicotine Alliance are a charity funded exclusively by consumers and represent them, they would be a great point of contact. A consumer only org eliminates possible issues with manufacturer or even tobacco company influence. The Government is aware that vape flavours are an important consideration for adult smokers when seeking to quit smoking and it will carefully consider any restrictions to avoid unintended consequences. The primary purpose of the Tobacco and Vapes Bill is to reduce smoking rates by bringing forward a generational ban on the sale of tobacco, making it an offence for anyone to sell tobacco products to anyone born on or after 1 January 2009. This policy is not being implemented for vapes because the health advice is clear that vaping is less harmful than smoking; however, vaping is not risk-free and nor is the consumption of nicotine. https://x.com/JonathanFoulds/status/1829195343780819169 The tobacco part of the bill is irrelevant according to this, and economists everywhere, cigarettes are going away. By the time the generational ban has any effect, there will have been no uptake of smoking for some years, and thankfully that will result in faster reductions in death and disease. The Generational ban is too slow, no effect for more than 20 years, but thankfully, THR (tobacco harm reduction) will have more effect and way faster, it has already begun as above. Nicotinecauses addiction rapidly and can increase the risk of developing conditions such as cardiovascular disease, gastrointestinal disorder and more rapid development of some cancers. Giving up nicotine is very difficult, and withdrawal symptoms can include cravings, irritability, anxiety, trouble concentrating, headaches and other mental symptoms. Evidence also suggests that the brain in adolescence is more sensitive to the effects of nicotine, so there could be additional risks for young people. That is why it is vital that vapes are only used as a smoking cessation tool. Vapes are an effective quit tool for smokers, particularly when combined with behavioural support. Therefore, it is important that vapes remain accessible to adult smokers. The Government remains fully committed to the Swap to Stop scheme, which involves swapping cigarettes for vapes. This part is shocking, and awful both at the same time. The misinformation presented to government is terrible. There is no good evidence that nicotine outside smoking increases the risk of cardiovascular disease, in fact long term studies in Sweden show nicotine from Snus is not associated with increase in cardiovascular risk, nor with any sort of cancer. Since Snus has been popular for a long time the evidence is based on studies of the actual population, much more reliable than e.g. extrapolation from cell or animal studies. Would you provide the source of this disinformation (Cardiovascular desease, gastrointestinal desease, cancer risk), and who presented it, please? This is important, the government needs true and up to date information, and sources of poor/disinformation need to be tackled. Further there is good evidence that nicotine can treat some gastrointestinal problems, please may I have the source for your claim it is a cause. I present some peer reviewed papers below, none are industry funded. I can present more if you would like? https://academic.oup.com/ntr/advance-article-abstract/doi/10.1093/ntr/ntae193/7727428 "Despite different mechanisms of action, both ENDS and CCs attenuated on-going colon inflammation, enhanced healing and ameliorated recovery of injured intestines of DSS-treated mice and UC patients." Citation: Kastratovic N, Markovic V, Arsenijevic A, Volarevic A, Zdravkovic N, Zdravkovic M, Brankovic M, Gmizic T, Harrell CR, Jakovljevic V, Djonov V, Volarevic V. The effects of combustible cigarettes and electronic nicotine delivery systems on immune cell-driven inflammation and mucosal healing in ulcerative colitis. Nicotine Tob Res. 2024 Aug 5:ntae193. doi: 10.1093/ntr/ntae193. Epub ahead of print. PMID: 39101540. https://www.frontiersin.org/articles/10.3389/fimmu.2022.826889/full Analysis of several studies - some animal. In general, nicotine is beneficial in ulcerative colitis; in particular, nicotine transdermal patches or nicotine enemas have shown significantly improved histological and global clinical scores of colitis, inhibited pro-inflammatory cytokines in macrophages, and induced protective autophagy to maintain intestinal barrier integrity. Citation: Zhang W, Lin H, Zou M, Yuan Q, Huang Z, Pan X and Zhang W (2022) Nicotine in Inflammatory Diseases: Anti-Inflammatory and Pro-Inflammatory Effects. Front. Immunol. 13:826889. doi: 10.3389/fimmu.2022.826889 Acknowledgements: This work was supported by the National Natural Science Foundation of China (grant number 81903319), Natural Science Foundation of Guangdong Province of China (grant number 2021A1515011220), Administration of Traditional Chinese Medicine of Guangdong Province of China (grant number 20211008), Special Fund for Young Core Scientists of Agriculture Science (grant number R2019YJ-QG001), Special Fund for Scientific Innovation Strategy—Construction of High-Level Academy of Agriculture Science (grant number R2018YJ-YB3002), Top Young Talents of Guangdong Hundreds of Millions of Projects of China (grant number 87316004), the foundation of director of Crops Research Institute, Guangdong Academy of Agricultural Sciences (grant number 202205) and Outstanding Young Scholar of Double Hundred Talents of Jinan University of China. https://www.hindawi.com/journals/grp/2008/237185/ Smoking has a detrimental effect in Crohn's disease (CD), but this may be due to factors in smoking other than nicotine. Given that transdermal nicotine benefits ulcerative colitis (UC), and there is a considerable overlap in the treatment of UC and CD, the possible beneficial effect of nicotine has been examined in patients with Crohn's colitis. In this relatively small study of patients with active Crohn's colitis, 6 mg nicotine enemas appeared to be of clinical benefit in most patients. They were well tolerated and safe. PDF Version Citation: J. R. Ingram, J. Rhodes, B. K. Evans, and G. A. O. Thomas, Hindawi Publishing Corporation, Gastroenterology Research and Practice, Volume 2008, Article ID 237185, 6 pages, doi:10.1155/2008/237185 Acknowledgements: J. R. Ingram was supported by the Gastrointestinal Foundation Trust. SLA Pharma gave financial support to the project. The authors are indebted to Dr. J. T. Green (of Cardiff and Vale Hospitals Trust) who referred patients, and to Professor G. T. Williams (GTW) who performed all histological assessments. Regarding nicotine addiction, the DSM requires significant harm as well as the difficulty in stopping use, the safer forms of nicotine do not pose sufficient risk/harm by that definition. Tobacco when smoked certainly does pose sufficient risk, thus addiction is justified. Loss of autonomy is not sufficient harm, though it does require consideration, if it where caffine in coffee would be addictive, not the more reasonable dependency forming. For the dependency of nicotine, your information appears out of date, I will deffer to Karl Fagerstrom, world leading expert and inventor of the most used dependency test for nicotine. Karl Fagerstrom | 14 December 2013 "We used to believe that nicotine is very dependence producing, but the evidence suggests that there are a number of problems with this statement. For example, animals do not self-administer nicotine as readily as they do other dependence producing drugs such as amphetamine, cocaine, and heroin (Villegier et al. 2003); nicotine is a relatively weak reinforcer in human laboratory studies (Perkins et al. 2001); abstinent smokers seem to prefer a much reduced or nicotine free e-cigarette rather than other - often stronger - nicotine-containing products like gum; and although nicotine replacement treatment is an effective aid for quitting smoking, its efficacy is moderate even in doses that replace most or all nicotine from the cigarettes formerly used (Dale et al. 1995). There is very little to no evidence for the abuse of nicotine when not delivered in a tobacco vehicle." https://nicotinepolicy.net/authors/karl-fagerstrom/dependence-on-tobacco-and-nicotine/ The above link contains more information expanding on the above, with references. The Vaping Products Duty did not form part of the previous Government’s Tobacco and Vapes Bill. Taxation is the responsibility of HM Treasury, which ran a public consultation on the proposals for the duty from 6 March to 29 May. HM Treasury and HM Revenue and Customs are currently considering responses to that consultation. There are no plans to introduce any tax changes as part of the upcoming Bill. I hope this reply is helpful. Thank you for the reply, it remains to be seen how useful this conversation is, it depends on your willingness to accept the evidence. Evidence is changing rapidly in tobacco and nicotine, this was not always the case, for a long time tobacco was the only source of nicotine in popular use, now that has changed (for the better with safer products, mostly not from the tobacco industry of old, I would argue). Regarding the tax, it need to be considered alongside policy, it as proposed is a 'sin tax' and will result in significant increase in illegal sales as tax avoidance adds to profitability, thus crime and sales to youth, as well as dissuading adults who smoke cigarettes from switching to a product that is likely to save their life. I would remind you that 30% of vape sales are illegal, I have previously written to explain some ways to reduce the impact of vapes on the environment (by a significant ten fold) and at the same time allow regulated products to out-compete the illegal products (making illegal sales nonprofitable is the easiest/cheapest control). A link o my previous letter https://safernicotine.wiki/mediawiki/index.php/File:Email_to_appg_vaping_28th_Feb_2023.pdf Yours sincerely, Correspondence Officer Ministerial Correspondence and Public Enquiries Department of Health and Social Care --------------------------------------------------------------------- ---------------------------------------------------- Please do not reply to this email. To contact the Department of Health and Social Care, please visit theContact DHSC section on GOV.UK To receive news about DHSC: sign up to our monthly newsletter This e-mail and any attachments is intended only for the attention of the addressee(s). Its unauthorised use, disclosure, storage or copying is not permitted. If you are not the intended recipient, please destroy all copies and inform the sender by return e-mail. Any views expressed in this message are not necessarily those of the Department of Health and Social Care. Please note: Incoming and outgoing email messages are routinely monitored for compliance with our policy on the use of electronic communications. -- Richard Pruen <richard@pruen.co.uk>|reply from DHSC and reply sent]] | |||
[[File:20240908122716 FAO- Wes Streeting, Potential risk reductions.pdf|thumb|alt=Dear Wes Streeting, Given the abundance of poor information circulating in Parliament, I thought I should provide an easy to understand example of what a 95% reduction is risk product can do to cancer rates. Unlike the modelling and assumptions that appear to prop up the tobacco and vapes bill, I will provide real population data from Sweden (they started using a harm reduction strategy with snus years ago, enough that real world data is available). You can verify these graphs by visiting https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Main_Page The use of nicotine in Sweden is roughly the EU average at 22%, but much of that is a product that is similar in risk to vaping, snus is also 95% or better less risky than cigarettes. Sweden in allowing some uptake by young people has seen the reductions above, snus has substituted for a much more harmful product and overall risk has fallen dramatically as seen above. The 'not without risk' aspect of nicotine and vaping is massively overplayed, it is certainly less risky than alcohol. As you can see above so far the UK has avoided the surge in adolescent vaping seen elsewhere, there has been a rise, but according to the latest ASH data 0.8% of frequent (> once per week) users are tobacco naive, so most of the increase is diversion from smoking (a good thing since if you never inhale tobacco smoke, it cannot harm you). This begs the question; if it seems to be working, why fix it? Further restrictions will drive the product to illegal sales, and like has been seen in Australia, that results in more sales to youth, and less access for adults, exactly the opposite of the desired outcome. We already have an illegal market in oversized/over strength products roughly 30% of the market, changes will cause it to step up and supply more if it becomes profitable. Big hint here that the proposed 'sin tax' on nicotine is guaranteed to increase illegal sales. Is the tax take in the short term favourable, with the increase in illegal sales it will prompt, compared to maximising the savings to the NHS? I would strongly suggest not! Extending the swap to stop scheme, particularly to target older cigarette users will have a huge effect on the NHS, reductions like those in the Sweden graph above, would save more than 500 million a year (up to 1 billion, if we can match Sweden in 50% reduction in lung cancer). https://www.brunel.ac.uk/news-and-events/news/articles/How-much-could-the-NHS-save-if-people-had-healthier-lifestyles-Hundreds-of-millions-according-to-research#:~:text=One%20of%20my%20studies%20indicates,mouth%20cancer%20and%20heart%20disease. The reduction would help cut waiting lists by 2029 as you have promised, especially if targeting the older at risk population with swap to stop. The tobacco part of the tobacco and vapes bill, that won't have had any effect by that point, and it is likely by the time it does the cigarette market will have collapsed/changed beyond recognition. I am not sure about it collapsing, but it is becoming obvious that big changes are afoot, and it will not be good for Big Tobacco of old. I would like to ask you to be cautious of changing regulations that we already have, and that appear to be working. Also to ensure that any further measures are well though out. The tobacco generational ban, I don't think will do any vast harm at least, it might have been a really good idea if implemented 20 years ago. I would also draw your attention to this regarding misinformation https://safernicotine.wiki/mediawiki/index.php/File:Email_6th_sept_DHSC_reply.pdf I have to wonder if misinformation on vaping is from tobacco companies, since as above vaping is doing a number on them? It seems this misinformation is stated without evidence usually or highly speculative evidence (rodent studies that are unsupported by the real world data). However I am happy to provide evidence for what I have said, and welcome any questions you may have, please feel free to ask. Thank you for your time. -- Richard Pruen <richard@pruen.co.uk>|Email FAO- Wes Streeting, Potential risk reductions]] | |||
[[File:APPG for Responsible Vaping Call for Evidence Form - 10 October 2024.pdf|thumb|alt=APPG for Responsible Vaping Inquiry on Vaping – Autumn 2024 CALL FOR EVIDENCE Those wishing to submit evidence to the inquiry should use this form. Submissions should be sent by email to info@responsiblevapingappg.org by 31 October 2024. Responses to individual questions should be kept to 500 words. Supporting information and evidence will also be accepted (see section 6). The APPG for Responsible Vaping is committed to transparency. The names of those organisations providing evidence, together with their submission, will be acknowledged in the final report and made available on the APPG for Responsible Vaping website. Personal information will not be released. All information gathered will be treated in accordance with the APPG’s GDPR policies. The APPG for Responsible Vaping has no links, connections or other engagement with the tobacco industry. If any tobacco company provides a submission to the APPG inquiry, as per guidance on requirements of article 5.3 of the World Health Organization (WHO) Framework Convention on Tobacco Control (FCTC), it will not be considered. About your organisation Q. Please provide your name and the name of the organisation that you are representing including contact details. Please indicate if you are responding in a personal capacity. I am representing myself as a consumer Q. Please outline your organisation’s field of interest/area of expertise in vaping including the relevant sector you represent e.g. public health, retail, manufacturer, regulator etc. I am a consumer of vaping products, I wish to present a consumer view Key Lines of Inquiry 1. The health impact of vaping including current application and usage 1a. Please provide comment and evidence to show the health impact of vaping including how, when and by whom such products are used, and their effectiveness or otherwise. Vaping provides a vastly safer alternative to combustible tobacco, both for current cigarette users, and for anyone who would start using riskier forms of tobacco. 1b. How should the government and others in public health treat vaping as part of the Smoke Free 2030 strategy and other health interventions? Vaping has a vastly lower and different risk profile to tobacco, the rules for tobacco are suitable for tobacco only (due to the extreme harm, and long lead time to that harm). Vaping must be treated separately and law must reflect the fact that it is at least twenty times safer than cigarettes. The risk is actually substantially lower, given use over 15 years has shown little problem. Vaping is capable of displacing cigarettes from the market, this has already begun.1c. And what are the barriers to this happening at present and in the future? focus on the generational ban as the go to policy, this will not do anything in time for the 2030 strategy, and the vapes part of it needs to avoid preventing switching, and any further restrictions favour expanding the illegal market. 2. Challenges facing the vape sector, including youth access and the environment 2a. How should we tackle issues relating to youth vaping? Please provide details of your experiences and supporting evidence including examples of effective interventions or other work, including from other sectors or countries. What else should the government, regulators, retail and vape sectors be doing in this regard and what does an effective strategy look like? Youth are already prevented from legally purchasing vapes, and the uptake of regular use > 1 time a week is 0.8% and not trending quickly in any direction. Keeping legal vapes on the market and available more freely than illegal ones is key, illegal vapes will only be sold if profitable, the cheapest control for illegal sales is to have legal products that prevent illegal products being profitable. Vaping is at least 20 times safer than cigarettes, and has an off ramp in tapering, while use is undesirable, it is still very much better than cigarettes for those determined to use nicotine. 2b. How should we tackle issues relating to the environmental impact of vaping. Please provide comment and evidence on the effectiveness of the current environmental legislative regime, such as the WEEE Directive, whether this is fit for purpose or what changes need to occur. I wrote to APPGVaping before with some ideas here is the letter from 28th feb 2023 this would also help suppress the illegal oversize devices, and reduce waste by a factor of ten times. https://safernicotine.wiki/mediawiki/index.php/File:Email_to_appg_vaping_28th_Feb _2023.pdf 2c. What other measures or schemes could be considered to improve the environmental impact of vaping? Is there, for example, a need to consider innovative take-back schemes together with financial penalties or incentives on the consumer, retailer and manufacturer, and what is the role for government and regulators? disposables should be discouraged, having a rewarded return scheme, and improving the design. For example I released a metal free pod that the part thrown away is entirely safe to throw away, the two tiny graphite contacts are the only parts that do not biodegrade quickly https://x.com/PruenRichard/status/1729128256329154749 It is dedicated to public domain so anyone can use for any purpose. 2d. Will the government’s likely proposal to ban single use or disposable vapes be beneficial in tackling youth vaping and the environmental impact of vaping? Are there potential consequences that need to be understood and explored? Please explain and evidence yourcomments. No it will likely drive all disposable sales to illegal markets (30% is already oversized/strength disposables) This will result in easier availability to underage due to no age of sale law being followed and greater risk due to untested products. This needs to be considered, a ban will increase danger. 2e. How can challenges relating to the growth of the illicit vape market be addressed and what role is there for government, regulators, law enforcement, retail, vape manufacturers etc? The regulated legal market is the best way to ensure it is not profitable to sell illegally, this has zero cost to implement. Ensure legal products are desirable and useable enough and there is no profit in illegal products. 2f. In recent years, there has been a significant increase among smokers believing that vaping is as harmful as tobacco use. Why has this come about, what are the risks with this and how can such misconceptions be addressed and corrected? Media focus on harms. This needs media and facts targeted particularly at older adults to get them facts and encourage then to switch as soon as possible. There is no other policy that can reach the most at risk population, older adults facing smoking related issues, the sooner they switch the better. 3. The economic impact of vaping towards public health, retail sector and wider economy 3a. What evidence can you share that highlights the economic impact of vaping, both positive and negative, towards the various sectors listed above. Having it be cheaper for the consumer is another reason to switch, the risk reduction is enormous so a large incentive is warrented to incentivise switching. 3b. What impact will the government’s likely course of legislative action (proposed ban on single-use vapes, banning advertising and branding as well as potential restrictions on vape flavours and retail display) on vaping have on the economic impact of vaping? Youth regular vaping is 0.8% and it might reduce that to 0.5% at best, meanwhile it will prevent many adults from switching, the adults still smoking face death 50% of the time. None of the youth starting will face death from vaping in the short or medium term, and unlikely to face death in the long term. The youth gain little for a lot of adult death. An annoying dependence VS 50% chance of death, these need to be weighted properly. 4. Proposed government legislative measures including flavours, packaging, display, excise and a ban on certain vaping products 4a. Please comment on the government’s likely proposed measures for regulating the vapesector including a ban on single-use vapes and a graduated excise regime – please indicate where you support or oppose such steps and your views on their likely consequences. as above the risk to youth and adults must be propperly considered. The risk of increasing illegal sales as well, it can be seen from Australia that demand exists and supply will meet it. Far better legal regulated vapes than illegasl ones. Flavours are vital for adults and any youth determined to try vapes will use whatever is available, it is unlikely to change the decision they make. 4b. Please comment on the government’s potential measures around packaging, display and flavours – please indicate where you support or oppose such steps including your views on their likely consequences (the APPG recognises that the government is still to publish full details around a number of these measures). Packaging/flavours should be no more restricted than the far worse alcohol, or other adult goods, if age of sale is acceptable for alcohol, and yet deaths occur in under 18s then a product without deaths and unlikely in the extreme to cause any, it doesn’t make logical sense. one puff in 30 days but 0.8% regular use indicates vapes are not as sticky as cigarettes, as most trials do not proceed to regular use. Risk reduction, because risk elimination is not possible. 4c. What are the risks, if any, to achieving the government’s Smoke Free 2030 ambition with its likely course of legislative action? The potential to increase the share of illegal sales, thus increasing availabity to youth, while causing adults to thing vaping is as harmful as cigarettes. Restrictions have a huge potential to cause harm, and little to do good on a whole population basis. 5. Better regulating the vape sector in the UK 5a. Please set out what in your view what would constitute a better regulated vape sector, with reference to examples from other sectors or countries. Where available, provide evidence to highlight how a particular route or measure has achieved its goals in delivering better regulation and the desired outcome. This could include responsibilities for government, regulators, retail and manufactures and both legislative and non-legislative routes. The existing rules are not too bad, they have led to the lowest youth vaping in the world and no spike in use as seen in the USA. Better enforcement of age of sale and keeping the illigal market suppressd, it would be very easy to do worse than continue as things are. 5b. Would a licensing scheme for vaping provide a better regulated sector and how could such a model work? Please provide any evidence to substantiate your comments including examples from other sectors or countries, and what would specifically need to occur to make this a feasible & effective scheme? 500 words No vapes should be available wherever cigarettes are available and with preferably less restrictions. The existing laws are good as they are, slightly favouring display of vapes over tobacco. Restrictions on vapes will make tobaccomore appealing in comparison, and tobacco is 20 times worse. 6. Other 6a. Please use this space to set out any other information or comments that you like to submit that you do not feel have been adequately covered by the above. Respondents can also submit an attachment. 500 words general supporting evidence attached Youth vaping is well under control and there are no sudden or worying trends or fad use. This is possibly as good as it gets, more restrictions are lilkey to make things worse (increasing illegal markets) Regular use very low and has been the same for several years|Response to APPG call for evidence]] | |||
[[File:Email-response-reply-DHSC-26-oct-2024-draft2.pdf.pdf|thumb|alt=Thank you for the reply, please find my response inline. On Thu, 2024-10-24 at 17:26 +0000, Department of Health and Social Care wrote: > Our ref: DE-1529395 <cut> We also remain fully committed to our Swap to Stop scheme, which sees up to one million adult smokers being encouraged to ‘swap to stop’, swapping cigarettes for vapes under the national scheme – the first of its kind in the world. Very glad to hear this, as suggested before I hope you would consider putting extra focus on reaching older cigarette users, they are the group most directly facing health harms, and the generational ban does nothing for them ever. The possibility exists to eliminate a huge amount of disease and death. With savings to the NHS year on year because cancer treatments are expensive. On the subject of the tobacco and vapes bill, I don't see the big rush the likes of ASHuk promote, by the time the legislation has any effect the 2030 smoke free deadline will have passed. IMHO it is better to take the time and get it right, than to rush through damaging regulations. Clive Bates provides good reasons here: https://clivebates.com/uk-tobacco-and-vapes-bill-a-misfire-and-a-backfire/ In addition, NHS programmes delivering nicotine replacement therapy are helping thousands of adults each year to live healthier lives with adult smoking rates dropping by more than half in the last three decades. Good, the more low risk options available the more likely people will find an acceptable one, and thus not die. Whilst vapes can be an effective quit aid for adult smokers, we are concerned about the worrying rise in vaping among children, and there are legitimate concerns about the unknown long-term harms from vaping. There has not been a significant rise in regular use of vapes (once a week or more) certainly nothing sudden or panic worthy. The Please see this graph: With 20 years of use, biomarker data, 16 years of popular use mostly in ex cigarette users, you are vastly overstating the remaining risk. Vaping is not likely to cause cancer of any kind (cancer potential 0.004% of smoking, a robust body of evidence https://safernicotine.wiki/mediawiki/index.php/Nicotine_-_Myth_-_Nicotine_Causes_Cancer) At this stage any possible risks are sure to be minor, the type that may cause discomfort or be annoying, but extremely unlikely to be life threatening. Science has moved on since cigarettes where found harmful, there is also real world population data from Sweden on reduced risk products and the effect. No need for modelling, there has been enough time to see the results in the eurobarometer. Vapes can do the same in the UK, or legalise Snus and copy Sweden, either way would work. As long as the you do not ban the good, while trying to achieve the perfect (resulting the disaster of more cigarettes). Ideally legalise Suns alongside vapes and transition those who will not vape to that, and cut deaths faster. Disposable vapes play a significant role in driving youth vaping with 54 per cent of current vapers aged 11-to-17 in Great Britain using them. They are easily available, cheaply priced and come in enticing colours and flavours. Additionally, they cause significant environmental harm with five million disposable vapes being either littered or thrown away in general waste every week. Given the level of environmental harm, the Department for Environment, Food and Rural Affairs is reviewing proposals to restrict the sale and supply of disposable vapes and will shortly outline its plans. Reusable and refillable products will remain available to help support smokers to switch and we do not have any plans to restrict vapes, for instance, to prescription only channels. There is absolutely no reason to punish the thousands of adults who will be put off from vaping, for 54% of 0.8% (youth vapers who never used cigarettes). Half of those adults not switching will die, while the youth will need to taper off nicotine using refillable vapes built in off ramp, cigarettes do not have that. Meanwhile according to NHS digital 2022 (graph below) 8% of 11-16 year old's have been drunk 3 or more times, vape are very effectively kept out of young peoples hands compared to that. There is no mass moral panic about alcohol, alcohol is far more deadly than vapes You need to sort priorities out, because the evidence doesn't support the focus on vapes. Enforcement of our regulations is vital. This is why we will ensure that the Tobacco and Vapes Bill contains new powers for trading standards, to take more immediate action to prevent the sale of vape to children and stop illicit products. That is great, underage sales need to be kept low, so does the illegal sale of unregulated vapes. In addition to local enforcement action, we are also providing £3million of funding over two years for Operation Joseph to reduce the sale of illegal vapes and nicotine containing vapes to under 18s. Operation Jospeh has been increasing funding at ports to ensure trading standards can conduct large seizures of illicit vapes before they enter the country. Great, but ensuring a legal market of products people want and find acceptable will mean illegal sales are unprofitable, there is also no cost to the government to enforce that. Restricting adults choices of flavours and full plain packaging will result in demand, the proposed sin tax will increase profitability, Australia at the time of writing has had 130 firebombings in the vapes turf war, do not bring that sort of insanity here, learn from their mistakes. Marketing is already restricted, and no reputable company targets underage users, they would be boycotted out of existence by consumers because they will not put up with youth targeting (I have seen this several times and it is very effective). Any genuinely youth appealing marketing or packaging can be dealt with under existing rules against advertising the product. It is while consumers are on side you can rely on this, if like Australia restrictions mean the public support the illegal market, then things will go badly here, just like Australia. I also worry the focus on vaping will detract from youth alcohol and drug prevention. Both these cause significant deaths, vaping doesn't even intoxicate, nor will it cause young people to die. The Department has previously published a call for evidence, a policy paper and a response to the public consultation on tobacco and vaping measures. All of these contain published links to evidence the Government has used in formulating policy and are relevant to many of the points you have raised. In addition to this, we work closely with organisations such as Action on Smoking and Health, public health bodies, academics, local organisations and other relevant parties to ensure that policy is based on the most reliable evidence. With respect it would be best to rely more heavily on the reports that where done for OHID, and less on hearsay or anecdotal evidence that may be brought up in parliament. Views should be heard, but must never take precedence over a report based on evidence and backed by science. We will be undertaking further consultations before the introduction of vaping regulations once the Tobacco and Vapes Bill has completed its parliamentary stages, and I would encourage you to respond to those consultations when they launch. Yes thank you. You can be sure I will be taking part in such consultations where possible. I am however just a consumer and care for my Mum who has vascular dementia, I hope this reply is helpful. Yes thank you, it makes it clear that risk is not an easy concept, and I hope the information presented helps to provide better perspective. Please feel free to ask any questions I will do my best to clarify any points or provide extra evidence if needed. Yours sincerely, Correspondence Officer Ministerial Correspondence and Public Enquiries Department of Health and Social Care --------------------------------------------------------------------- ---------------------------------------------------- Please do not reply to this email. To contact the Department of Health and Social Care, please visit theContact DHSC section on GOV.UK To receive news about DHSC: sign up to our monthly newsletter This e-mail and any attachments is intended only for the attention of the addressee(s). Its unauthorised use, disclosure, storage or copying is not permitted. If you are not the intended recipient, please destroy all copies and inform the sender by return e-mail. Any views expressed in this message are not necessarily those of the Department of Health and Social Care. Please note: Incoming and outgoing email messages are routinely monitored for compliance with our policy on the use of electronic communications. -- Richard Pruen <richard@pruen.co.uk>|Email response to DHSC draft 2]] | |||
[[File:Email-dhsc-20-nov-2024.pdf|thumb|alt=Hi folks, Since the government promised to be evidence led, I thought this new evidence was vital for vaping policy. In this paper the authors examined respiratory symptoms in e-cigarette users without a history of smoking from the VERITAS cohort. While vapers reported slightly more frequent symptoms than non-vapers on the Respiratory Symptom Experience Scale, the difference was not clinically significant. Disposable e-cigarettes were the most common device type, with fruit flavors preferred by most users. https://www.nature.com/articles/s41598-024-80221-8 The VERITAS cohort https://veritascohort.coehar.org/ aims to provide long term data on vaping in never cigarette users <100 cigarettes in their life, and is important because most vapers are past cigarette smokers and significant confounding exists due to this. The first data above shows 'the difference between groups was not clinically significant', further proof that in the long term, vaping is vastly safer than smoking, and the effects on non-smokers are tiny, not clinically significant. It is vital that you factor this information into policy because adults who are convinced not to switch face death 50% of the time. Adolescent nicotine use is falling, and if they do use any product, then smoking should be the least available to them, as it is the most harmful. Vaping in adolescents is lower than alcohol use, and alcohol is far more toxic in both the short and long term. The current age of sale laws means the UK has the lowest regular use of vapes in underage in the world; we should keep doing that, but be aware that there is little harm from vaping when you compare that to the death faced by cigarette smokers. The tax and ban policy will not work; it will lead to illegal markets, just like Australia has seen; once control is lost, it will be harder to regain. Sweden, on the other hand, did not reduce nicotine use, which is average for the EU, but has seen reductions in smoking-related diseases and cancer. They have also achieved the smoke-free goal 17 years early: The UK will reduce death and disease more rapidly being more like Sweden than like Australia. I would like you to focus on reducing death and disease quickly, and without sacrificing the older cigarettes smoking population, this is possible, if Sweden can do it, so can the UK. Thank for your time. -- Richard Pruen <richard@pruen.co.uk>|Email to DHSC 20 nov 2024]] | |||
DRAFT: [[File:Letter minister for health 11th Feb 2025.pdf|thumb|alt=Subject: Ongoing Vaping Policy Dear Ashley Dalton, I am contacting you as a vaping consumer and advocate for saving lives; vaping saved my life (I am happy to share medical records to prove that), and I aim to pass that on to as many as possible. I am not paid in any way by anyone to do so. I have worked in the vaping industry, helping to develop standards and testing against them (I ran BTC battery testing until 2016). This was good for consumer safety, but the industry did not necessarily favour it. I am also part of a group funded by ASH advocating for smoking cessation in people living with severe mental illness; 40% smoke cigarettes, double the national number. I was disturbed to hear some of the testimony given in parliament. Much of the information was incorrect or deliberately misleading. You must do better when debating a serious health matter; accurate and science-backed information is critical to saving lives. You should use the research OHID paid for using taxpayers' money, not anecdotal (often second-hand) accounts from teaching staff or parents frightened by the media. Consumers are not represented; I would ask you to consider involving NNA (New Nicotine Alliance) as they are a consumer-only group that is not funded by the industry. info@nnalliance.org Charity Registration Number: 1160481. It seems fair since UKVIA (industry trade association) and tobacco control NGOs were involved, but there was no one for consumers. Sadly, the media is almost all negative and presents harm because that sells papers; the truth is that in 12 years of monitoring by the MHRA yellow card early warning system, not one single disease/symptom has been detected as linked to vaping nicotine. There have been less than 20 admissions to hospital per year, and none fatal, compared to 15 per day for household cleaners (some sadly fatal). I agree that you should keep a close eye on frequent vaping among adolescents; thankfully, that remains low and does not show worrying trends (see graphs below). Experimentation with vaping is preferable to cigarettes, and still, too many are starting to smoke tobacco. Unlike tobacco, vaping is unlikely to cause deaths since 20 years of study shows no such issue. Vaping has (with open devices) the off-ramp of tapering nicotine slowly (around a third of folks quitting smoking with vapes also stop vaping this way; see ONS data that you must have access to). It is essential to accept the vastly lower risk from vaping when considering legislation that will steer adolescents in a particular direction. Assuming they will do extra homework if they can’t experiment is faulty. They will likely do something more risky instead, such as alcohol. Alcohol, for example, results in accidents, intoxication and deaths. This is sadly human nature, and harm reduction at least keeps the risks as low as possible. It is also vital to ensure that illicit vapes and illegal tobacco sales are kept to a minimum; buying vapes from ‘dealers’ opens all manner of unwanted possibilities, including other more harmful illegal drugs offered at the same time. Thus, great care is needed to avoid a ban on a product type resulting in supply shifting to criminal-controlled illicit sales. Australia is a perfect example of open gang war and fire bombings. A legally regulated market that renders illegal supply unprofitable is the best solution; there is no enforcement cost in that case, and consumers should be protected against entirely unregulated products. In Sweden, the use of nicotine is about the same as in the EU as a whole, but the rates of cancer are lower, particularly in men, since they switched earlier, and the trend is now apparent in the data. It is worth looking at Sweden because it has had a harm-reduction product for a long time, and trends and population data are readily available. It is obvious that nicotine is not the problem; combusted tobacco is the killer, particularly cigarettes; switching existing users to safer products is the priority; you can save vast numbers of lives and treatment costs. I suggest you research the history of THR in Sweden, allowing users to initiate nicotine use with a safer product works; they have the lowest cancer rates in the EU by a good margin. (see the following graphs) The UK can still do the same with vaping by not restricting it too much. Yours sincerely, Richard Pruen|Letter minister for health 11th Feb 2025]] | |||
[[File:20250413114422 Cigarettes and Big tobacco.pdf|thumb|alt=I thought this Sobering analysis of the US cigarette market might be interesting. It looks like Big Tobacco is winning, while the only successful commercial alternative (vaping and other THR (tobacco harm reduction) products like tobacco-free pouches) are being further restricted. The UK is falling into the same trap. "Last August Barclays analysts updated the data to show how US cigarettes had become massively more profitable. Based on that Goldman Sachs report this week, the ever-accelerating price increases since last August will bring the gross profit on a pack of Marlboros to $4.50 and the operating profit to around $3.64. More than doubling profits per pack in less than five years, and on a product that costs a mere 40 cents to make." The entire report by David Sweanor, a well-known tobacco control expert from Canada, is attached. While no one wants young people to take up vaping, it is far more vital that they do not start smoking cigerettes. Youth vaping once a week or more is low and remains so (please see graph) The current government plans for a smoke-free generation will not help anyone currently smoking cigarettes; they also have the significant downside of forcing any young people insisting on using nicotine into the illegal market; the sin tax on legal vaping will mean the cheapest/most available product they encounter will be illegal cigarettes, likely they will use those. As we are well aware, cigarettes are not safe, and they are not better than vaping. Despite the ridiculous claims of the press and the rubbish spouted in Parliament, vaping has not been linked to any disease or syndrome. Twelve years of MHRA early warning monitoring would have detected anything serious (that is the reason for its existence). The data is available here: https://safernicotine.wiki/mediawiki/index.php/MHRA_yellow_card (or ask the MHRA). This government promised to be evidence-led, so please look at the evidence and do that. The overabundance of caution to prevent youth vaping will cause more youth to start smoking cigarettes, and that cannot be a good thing; it will cost lives. I would ask you to consider carefully because THR can save at least some of those lives. It may not be perfect or easy to regulate, but lives are important. I do not want to be able to say 'I told you so', I would much rather you did better and saved more lives, please! |Letter to DHSC 13 April 2024]] | |||
Latest revision as of 16:31, 13 April 2025
| Babel user information | ||
|---|---|---|
| ||
| Users by language |
The Site admin
Richard Pruen
Electrical and electronic engineer
Favorite band: Rush
Why spend so much time on this? It’s a fact that nicotine harm reduction (vaping and Snus) saved my life, this is my way to pay that forward, and pass along information on safer nicotine.
Running a site from the ground up, has proved interesting and worthwhile. Some of the things I have learned about Linux, and configuration of software for servers is only stuff you learn by doing.
I suspect the site will stick around, at least as long as it is required to provide links and info.
I might well put more info of my vaping / thr story here soon, this is just a test edit.
More test edit, and added some features, like babel to indicate users languages.
Site admin at Safer nicotine wiki.

ABOUT
Ecig user since 2008, consumer advocate for vaping and THR #VapingSavedMyLife #VapingSavesLives
Twitter @pruenrichard
Below are letters and documents sent in advocacy efforts as a record and should anyone wish to use them for ideas. These are my efforts and do not necessarily reflect the views of the wiki or other users.





![Response ID ANON-EJTE-W3QH-B Submitted to Proposed reforms to the regulation of vapes Submitted on 2023-09-08 21:15:44 Survey contents Privacy and your personal information I consent to the TGA collecting the information requested in this survey about me, including any sensitive information, for the purposes indicated above. Agree: Yes Acknowledgement I agree. Yes.: Yes Introduction 1 What is your name? Name: Richard Pruen 2 What is your email address? Email: richard@pruen.co.uk 3 What is your organisation name? Organisation name or N/A: n/a 4 Please choose a stakeholder group that best describes you or your organisation. Others* *If other, please specify:: Consumer 5 Which best describes your response? I am responding as an individual. 6 Are you an authorised prescriber? No (please go to next page Conflicts of interest (actual or perceived) 1 Have you or your organisation ever received services, assistance or support (whether monetary or non-monetary in nature) from the tobacco industry and/or e-cigarette industry? If this scenario applies to you or your organisation, please provide relevant details in the textbox. Yes If you have selected yes, please provide details here. Otherwise, please state 'Not Applicable':: I owned a company testing electronic cigarettes for compliance with UK and other standards, as well as carried out investigations of failures including battery failure. I also worked on R&D and provided consulting services on for example battery protection circuits, chargers etc. Payment was from user fees for testing, government agencies (trading standards), trade associations, and sometimes individuals or companies carrying out due diligence testing or failure mode analysis. Ended 2016 since then I have been a consumer only and have not received any funding from any company (of any sort), government agency, or researchinstitution. 2 Have you or your organisation ever provided services, assistance or support (whether monetary or non-monetary in nature) to the tobacco industry and/or the e-cigarette industry? If this scenario applies to you or your organisation, please provide further information in the textbox. Yes If you have selected 'yes', please provide details here. Otherwise, please state 'Not Applicable': I assisted in writing standards for UK vaping products (PAS 54115 A guide for the importation and sale of electronic cigarettes and directly related products, with product safety testing methods) and proposed an IEEE standard project number P2800. Several sampling machines were supplied to others testing electronic cigarettes, and other custom test equipment, the supplied equipment presumably used to carry out tests on electronic cigarettes as designed. As academic and test houses purchased this equipment it is assumed this was paid for by test fees, or grants to carry out tests on electronic cigarettes, again possibly linked to taxes etc from tobacco and or electronic cigarette sales. The same funding source as government agencies, politicians and others working in the field. Again since 2016 I have been a consumer only. Proposal 1 -Restrictions on importation, manufacture and supply of all vapes . 1 Do you support the proposed approach to ban disposable single use vapes absolutely and all other vapes, except those for legitimate therapeutic use in compliance with the TG Act? No 2 How would you anticipate industry and consumers to respond to a ban on the importation, manufacture and supply of non-therapeutic vapes? * Please provide answer here. : Demand will remain, along with the risk of vaping being seen as cool because it is something disallowed. The tightening of rules is unlikely to be enforceable, so illicit supply will continue to be the primary supply to the population. The population know vaping is safer than smoking, thus it will be very difficult to curb demand. Prohibiting drugs such as cocaine and cannabis fails, vaping prohibition will almost certainly follow the same pattern. 3 Do you support removal of the personal importation scheme exception for vapes? If not, what would be the impact on you? No (* if not, what would be the impact on you?) * What would be the impact on you?: Vaping products that are acceptable and usable are likely to only be available via illicit sales, and criminal gangs. Particularly as research shows flavours to be vital for the prevention of release to smoking. These products will not be tested or regulated in any way, importing allows users who have a prescription to import what they need to stay smoke-free, thus not relapse to smoking and potentially death. Importantly importing from somewhere with a regulated legal market, they can be sure of the quality and contents of the products they buy. The one-size-fits-all approved vapes that consumers will find at pharmacy outlets is unlikely to be effective since most of the features that make an effective substitute for cigarettes will be regulated out. 4 Do you agree with the proposal to retain a traveller’s exemption, including the proposed limits? Yes 5 Do you support the proposed approach to prohibiting the advertisement of all vapes (subject to limited exceptions)? No 6 [If applicable] Suppliers, what part of supply chain do you occupy? Not applicable * Other -specify your role in supply chain.: Consumer 6 (a) What proportion of your sales volumes is attributable to vape sales [i.e. quantity of vapes sold]? Please provide details here: (or mark Not applicable).: N/A6 (b) What proportion of your sales revenue is attributable to vape sales [i.e. revenue earned from sales]? Please provide details here: (or mark Not applicable).: N/A 6 (c) What impact would the proposed measures have on your sales volumes? Please provide details here: (or mark Not applicable).: not a vendor, none 6 (d) What impact would the proposed measures have on your sales revenues? Please provide details here: (or mark Not applicable).: none not a vendor 6 (e) What proportion of your vapes sales is attributable to disposable single use vapes versus refillable products? Please provide details here: (or mark Not applicable).: not a vendor 6 (f) How would restricting the importation, manufacture and supply of disposable single use, and non-therapeutic, vapes in Australia impact you? Please provide details here: (or mark Not applicable).: not a vendor N/A 6 (g) How much stock do you have in Australia currently and how long would it take to sell that stock? Please provide details here: (or mark Not applicable).: not a vendor N/A 6 (h) What would be the cost to you if you were required to dispose or otherwise move on existing stock? Please provide details here: (or mark Not applicable).: N/A Proposal 2 -Changes to market accessibility requirements, including better regulation of device components. 7 Do you support the approach to require a pre-market notification of compliance with TGO 110? No 8 [If applicable] For suppliers of therapeutic vapes, what impact would the proposed notification system have on your supply model and what transition period would you require to comply with the new notification requirement? Please provide details here: (or mark Not applicable).: not a vendor 9 Do you support the proposed access to vapes under the SAS C notification system? No 9 (a) What impact would this pathway have on facilitating patient access to therapeutic vapes? Please provide details here: (or mark Not applicable).: Vaping works in the rest of the world as a product substitute, providing a safer alternative to a deadly (cigarettes) product. In the UK and NZ smoking decline has accelerated significantly past that in Australia, due to the adoption of consumer vaping, slightly less so in the US where the regulator is not so certain. The prescription model in Australia has failed, smoking has not continued to decline and may have increased possibly. Vaping is also higher in Australian youth than UK and NZ, the current policy has backfired and should be reversed. It is absolutely obvious at this point that unless you have unlimited resources for enforcement, the current policy is not workable, and never will be. The time has come to use what has worked elsewhere and start again.10 [If applicable] For prescribers, would the proposed new pathway likely change your approach to prescribing therapeutic vapes? How? Not a prescriber of vapes * How new pathway will change your approach to prescribing ttherapeutic vapes?: 11 [If applicable] For prescribers, which access pathway (SAS B, SAS C, or AP) would you envisage using to prescribe therapeutic vapes? Why? Not a prescriber of vapes Please tell us why: 12 [If applicable] For prescribers, would integration of SAS or AP applications or notifications into existing clinical software systems ease the administrative burden and/or encourage you to use the new pathway? Not a prescriber of vapes 13 Do you agree with the proposal to regulate both e-liquid and device components of unapproved vapes under the same part of the TG Act for simplicity? No 14 Will these changes have direct or indirect impact on you? Please provide details. Yes (please provide details below) Please provide details here:: As a consumer I want safer options to be available to me and to every person who smokes tobacco or would smoke tobacco for lack of a viable alternative. Sadly some kids will do adult things even if you try to stop them (for example drinking alcohol, unsafe sex, taking drugs, smoking) while they should not be encouraged to vape, it still offers a harm reduction if it diverts them from smoking, like it or not, this is true because safer is safer. 15 Do you require time to adjust to these requirements? If yes, how long? Yes 15 (a) How long do you require to adjust to these requirements? More than 12 months Proposal 3 - Improving quality standard for unapproved (unregistered) vapes) 16 Are the definitions of nicotine and mint flavours appropriate? If not, please provide reasons. No (* please provide reason below) * Please provide reason here.: Nicotine itself does not have a flavour, the flavour should be correctly referred to as "artificial tobacco flavour" There is no evidence that human flavour preference varies by age and none particularly that it changes at 18. It is therefore impossible to target age groups with specific flavours, thus limiting flavours on this basis has no merit whatsoever. 17 Do you agree with the proposed upper limit on the concentration of menthol in vapes? If not, please provide reasons. No (* please provide reason below) * Please provide reason here: It is trivial to add menthol to vapes, this simply encourages users to add more if they prefer, opening a can of worms and the potential for contamination or incompatible ingredients. This seem unwise for very little if any benefit. 18 [If applicable] Importers, manufacturers and suppliers, would the restrictions on flavour proposed above impact you? Not applicable 19 Do you agree with the proposal to require pharmaceutical-like packaging and presentation for vapes, e.g., vapes manufactured in black, white or grey coloured materials, predominantly white background on packaging, clear warning statements and other restrictions on labels in addition to other selective TGO 91 requirements for vapes? No (* please provide reason below)20 [If applicable] What impact will the labelling and packaging changes have on you? * Please provide detail here.: It will probably backfire, making legal products undesirable is likely to increase the number of people using illicit products, particularly if access remains easy, without enforcement that is most likely to be the case. 20 (a) How long would you need to transition your product to comply with the proposed requirements? More than 12 months 21 Do you agree with our approach to allow only permitted ingredients in vapes, instead of trying to prohibit individual chemical entities from use in e-liquids? No 22 [If applicable] Importers, manufacturers and suppliers, will your therapeutic vapes need any re-formulation or other changes to comply with the permitted ingredients and ingredient quality requirements? Not applicable 22 (a) If product re-formulation is required, how long will you need to make these changes? More than 12 months 22 (b) If product re-formulation is required, what financial or business impacts would be associated with them? Provide detail here or put 'Not Applicable': Not a vendor 23 Do you support applying the same regulatory controls to zero-nicotine therapeutic vapes, as for NVPs? No 24 What is the overall business cost on you to comply with a strengthened TGO 110? Please provide details here: (or mark Not applicable).: not a vendor 25 Do you agree with the proposed requirements under TGO 110 that will apply to unapproved device components of vapes? No 26 [If applicable] Suppliers, do you intend to register any vaping device on the register as an approved medical device? No (if no, why not?) If no, why not?: not a vendor 27 [If applicable] Importers, manufacturers and suppliers, are you familiar with relevant US FDA, or MHRA guidance and/or EU standards covering vaping devices? Not applicable 27 (a) Do your vapes currently comply with relevant US FDA, or MHRA guidance and/or EU standards covering vaping devices? Not applicable 27 (b) If not, what requirements do you meet? What requirements you currently comply with?: not a vendor 27 (c) How long would it take to achieve compliance with relevant standards? More than 12 months28 [If applicable] Importers, manufacturers and suppliers, are your vapes manufactured at facilities that hold relevant international standards for Quality Management Systems, such as ISO9001 or ISO 13485? Not applicable Proposal 4 - Strengthening domestic compliance and enforcement mechanisms 29 Do you have any other comments in relation to this proposal? Yes (* provide your comments below) Comments: I reiterate that Australian policy has failed, and further moves in the same direction are likely to fail. Other countries have shown much more desirable results, the best results on smoking have been where vaping has been accepted as a consumer alternative to smoking, but the prescription model, unfortunately, has proven unworkable. Realistically you should review the past responses to enquiries, select a number of people who have successfully predicted the results of current regulations, and ask them for solutions. At least they have a track record, and proven knowledge of the real world and likely outcomes. Supplementary questions 30 [If applicable] Suppliers, please confirm if you intend to continue to supply therapeutic vapes under the proposed reforms described? Not applicable * Product range : Not a vendor, but as a consumer, I can see vendors dropping out. This will benefit the criminals and gangs who supply illicit markets, more trade for them. 30 (a) How long would it take to meet the new requirements? More than 12 months 31 [If applicable] Suppliers, please confirm if you intend to register your therapeutic vapes in the next 2 years? Not applicable What guidance and/or clarity of supporting data requirements do you need from TGA: not a vendor Publication of submissions To proceed, please select from the options below how you would like the TGA to deal with your submissions: I agree to the TGA publishing my response in full. I request the TGA to consider redacting sensitive commercial information from my response before publication: No Please specify sensitive commercial inforation you want redatced :](/mediawiki/images/thumb/8/8b/TGA_consult_8-sept-2023_my_response.pdf/page1-300px-TGA_consult_8-sept-2023_my_response.pdf.jpg)


![Subject: COP 10 WHO FCTC Dear Rosanna O’Connor, I am a consumer advocate for vaping, and do not use disposables beyond experimenting to see what they are like. I am also an engineer. I have worked in the vaping industry previously testing compliance with the standards for vaping products, and owned a now closed company BTC Battery Testing LTD (closed 2016). Currently I care for my mother who suffers vascular dementia, and as such volunteer my spare time to the cause of Tobacco Harm Reduction. I believe that consumers should be present at the COP 10 meeting, it is consumers who have the most to gain from stopping the use of combustible tobacco, and the lived experience of trying to do so. Many millions have found a way to eliminate almost all the risk via THR products. The phrase ‘Nothing about us without us’ springs to mind. Why then are the public and press excluded. I would like to see the proceedings live streamed, so those effected can see what is being done. In no way could this effect the discussions, thus is reasonable transparency. I would like an answer regarding the possibility, please. Many countries already found harm reduction useful, critical even. Be that low risk Snus (Sweden has the lowest cancer rate in Europe, and will be smoking free this year (>5%)). Vaping that the UK NHS finds almost 66% effective with support, as stated on their website. New Zealand has seen similar results, especially in native populations, reducing disparities. Japan has seen huge drops in cigarette sales due to reduced harm heated tobacco products. Please see the letter from the Lancet from Robert Beaglehole and Ruth Bonita. They were both senior officials at WHO and are now at the University of Auckland. Robert was formerly Director of the Department of Chronic Disease and Health Promotion at WHO. Ruth was formerly the Director of Surveillance in the Noncommunicable Disease Cluster at WHO. I wish to add my support for their recommendations, the article is attached (also link here https://doi.org/10.1016/S0140-6736(24)00140-5) please make sure these points are discussed at the COP 10 meeting. Yours sincerely, Richard Pruen P.S Please ensure the representatives listed on the next page can discuss before the metting and forward more widely if you agree with the sentiment. Katherine Sands Tobacco Control Team Leader Department for Health and Social Care Martin Dockrell Tobacco Control Programme Lead Department for Health and Social Care Alison Walker Senior Tobacco Control Policy Lead Department of Health and Social Care Esther Lawrence Deputy Head of Global Health UK Mission to the UN, Geneva Please find attached a letter from [THELANCET-D-24-00371] S0140-6736(24)00140-5](/mediawiki/images/thumb/4/4f/Letter_to_cop_10_repersentitives.pdf/page1-300px-Letter_to_cop_10_repersentitives.pdf.jpg)






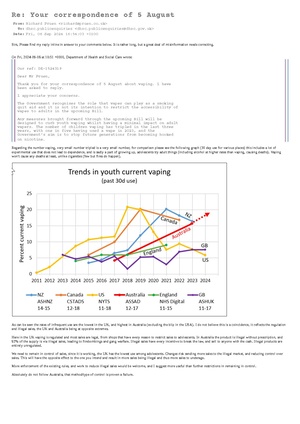




DRAFT:

