Nicotine - Stigma
Jump to navigation
Jump to search

Stigma and stigmatizing language lead to viewing people as less worthy and can lead to bias and discrimination. Stigma can affect the mental health of the stigmatized, may inhibit their ability to achieve wanted changes in their lives, and may cause them to avoid medical care or helpful services. This page explores the use of Person-First Language and the consequences of stigmatizing people, with a focus on those who use nicotine.
Smoking (Nicotine) Stigma and the use of "Smoker"
Publication Policies/Author Guidelines - Person-First Language (PFL)
Mentions "Smoker"
2021: ACS/ACS CAN: Inclusive Language and Writing Guide
- Terms to avoid: smokers/former smokers
- Suggested Replacement: people who smoke/used to smoke/ quit smoking
- Rationale: removes stigmatizing or shaming/blaming language and keeps people first
- 2023 AJPM Revision Guide: "Person-first language is used throughout (“people who smoke” preferred instead of “smokers”; “persons who use drugs” preferred instead of “drug users”, etc.)."
- Avoid Lung cancer patient. Preferred Patient/person with lung cancer
- Avoid Smoker. Preferred Patient/person with active tobacco use OR patient/person who smokes
- Avoid Nicotine addict Preferred Patient/person with nicotine dependence
- Avoid Former smoker Preferred Patient/person with smoking history
- Avoid Nonsmoker Preferred Patient/person who doesn’t smoke
John Hopkins Bloomberg School of Public Health: Bloomberg School Editorial Style Guide
- To avoid stigmatizing language, do not use these terms:
- smoker(s)
- tobacco [or other acceptable product term] user(s)
- non-smoker(s)
- never smoker(s)
- vaper(s)
- user(s)
- Use person-first language:
- person who smokes/people who smoke
- person who uses tobacco/people who use tobacco [or other acceptable product term]
- people who report no current smoking
- people who use heated tobacco products
- He has never smoked.
- She uses e-cigarettes.
- Do not label people with their condition.
- Avoid: alcoholic, addict, user, abuser, smoker, asthmatic, epileptic, obese.
- Preferred: people with opioid use disorder, person who smokes, individuals who have asthma, people with epilepsy, person with obesity.
- An exception to this guidance is in cases where persons prefer to be identified by a condition.
- Example: Deaf person, pregnant person.
Journal of the National Comprehensive Cancer Network (JNCCN) NCCN Language Guidance: Sensitive, Respectful, and Inclusive Language for NCCN Publications
- Patients should not be belittled or made to feel stigmatized by their age, their size, or their past or current behaviors.
- Individuals should not be defined by their substance use. Feeling stigma can prevent people with a substance use disorder from seeking treatment, and implicit or explicit bias of health care professionals can impact the care they provide to individuals with substance use disorders. NCCN publications use person-first language and avoid terms associated with stigma and negative bias when discussing substance use.
- Instead of "smokers," use "people who smoke."
- End Stigma: For example, instead of “smoker,” use “person who smokes.”
- Use Person-First Language: For example, instead of “lung cancer patient,” use “patient/person with lung cancer.”
- End Stigma: For example, instead of “smoker,” use “person who smokes.”
- Remember person-first language. Participant who currently smokes, not “smoker.”
Tobacco Control: New policy of people-first language to replace ‘smoker’, ‘vaper’ ‘tobacco user’ and other behaviour-based labels
- ..."Tobacco Control is instituting a new policy of people-first language when referring to people who use tobacco and related products. Terms such as ‘smoker’, ‘vaper’ and ‘tobacco user’ (and their various iterations) should no longer be used as general descriptors."
- "However, people-first language does not invalidate how people may choose to self-identify. It provides a broader conceptualisation which reduces the potential for stigma, resists tobacco industry narratives and promotes greater precision and accuracy, as well as creating space which recognises these self-claimed identities can change."
Doesn't Mention "Smoker" (Person (people)-First, Person-Centered, Person-Forward)
- Strongly recommends the use of “people-first language.”
- “Words Matter” - Guidance on Language and Terminology
- Please use “person first” language (e.g. “person/patient/participant with alcohol use disorder”, rather than “alcoholic”). Person-first language helps to reduce stigma against people who use drugs by not implying that they are their disorder. “Addict” and “alcoholic,” while often used among some patients and the public, can be stigmatizing, dehumanizing, and do not reflect the very human condition of addiction.
- Preferred terms for the disease include substance use disorder, alcohol use disorder, drug use disorder, gambling disorder, and addiction. Use of terms in other diagnostic systems are acceptable provided the terms are used as defined. Examples include “dependence” when referring to pre-DSM 5 or International Classification of Diseases (ICD) diagnoses, or the ICD diagnosis “Harmful Use.” Note that “drug” should not be used when the more appropriate term is “substance” (i.e., drug, alcohol, and tobacco) or “medication” (i.e., drug intended for medical use).“Person who uses drugs” should be used rather than “drug user.”
- "Authors should use “person-first” language..."
- Authors are encouraged to be thoughtful about the connotations of language used in their manuscripts to describe persons or groups. Person-first language (e.g., “persons with sexual offense histories”, “individual who has been adjudicated for…”, “child/adolescent with sexual behavior problems”) is generally preferred because it is often more accurate and less pejorative than terms like “sex offender”. Terms like “sex offender” imply an ongoing tendency to commit sex offenses, which is inaccurate for many persons who have been convicted for sex offenses given current sexual recidivism base rates. Similarly, the term suggests a homogeneous group defined and stigmatized on the basis of criminal behaviors that may have taken place infrequently or many years in the past.
- Authors should use inclusive and person-first language in manuscripts. Describe people as having a condition or disease, experiencing a circumstance, or doing something specific rather than the condition, disease, circumstance, or activity being part of their identity. For example, they should use “people with obesity,” “person with HIV,” “person who injects drugs,” and so forth, rather than “obese people” “HIV positive” or “drug user.”
- "In most cases it is preferable to emphasize the person over the attribute. For example, “person with cancer” instead of “cancer patient”, “man in prison” instead of “inmate.” Emphasizing the attribute can reduce the person to a label and dehumanize them."
- Strongly recommends the use of “people-first language.”
- Drug and Alcohol Dependence is committed to eliminating stigmatizing language by adopting "person forward" language when publishing reports of addiction science findings.
- The European Association for the Study of Obesity requires use of person-first language and non-stigmatizing images in all written and verbal communications.
- To the greatest extent possible, inclusive language should be used throughout the text. Authors are encouraged to use person-first language (e.g., "a person experiencing homelessness" rather than "a homeless person" or "patients with diabetes" rather than "diabetics").
- Authors are expected to use "person/people first" language (e.g., "individuals with chronic mental disorders" rather than "the chronic mentally ill").
- Journal of NeuroEngineering and Rehabilitation recommends the use of person-first language to speak appropriately about individuals with a disability. For example, when referring to a person with a stroke, refer to the person first using a phrase such as 'a person with a stroke' or 'a person who has a stroke'. Avoid terms such as 'victim', 'the handicapped', 'the disabled', or 'brain damaged'.
- People-first language, like “people with addictions,” “people in recovery,” and “people with substance use disorder” is preferable. Avoid terms like addict, substance abuse, junkie, and drug abuse
- Our language always respects the integrity and the individuality of the people affected by these illnesses. All NAMI documents and NAMI co-authored documents use language that puts people first. For example, "individuals living with serious mental illness" instead of "mentally ill people" or "the mentally ill"; “people living with schizophrenia” instead of “schizophrenics,” and "people who are not criminally responsible" instead of "the criminallyinsane."
- "Reference is to individuals with disabilities, not handicaps, handicapping conditions, or impairments. Authors should apply this person-first policy in their manuscripts."
- Person-first language, which emphasizes the individual or group rather than the condition, disease, or situation, should generally be used, eg, “child(ren) with diabetes” and “child(ren) with obesity” rather than “diabetic child(ren)” and “obese child(ren).” Exceptions to first-person language include certain identity-first language for individuals and groups who prefer it, eg, “Deaf child(ren)” or “autistic child(ren).”
- Prosthetics and Orthotics International requires that authors use inclusive language, conveying respect to all people and acknowledging diversity.
- When preparing submissions, authors are encouraged to use person-first language emphasising the person and not their disability. For example, authors should use terms such as “a person with an amputation” or “a person who has diabetes”, instead of “amputee” or “diabetic."
- Sage is committed to promoting equity throughout our publishing program, and we believe that using language is a simple and powerful way to ensure the communities we serve feel welcomed, respected, safe, and able to fully engage with the publishing process and our published content.
- Person-first language emphasizes the person. Examples:
- “person living with a mental health condition” instead of “mentally ill.”
- “person with a substance use disorder” instead of “addict.”
- Guidance for improving the language researchers use to talk to and about people with studied health conditions has been issued in several fields. The Editors of SLEEP® endorse the use of people-centered language in research communications. Our recommendations for people-centered language for sleep/circadian research publications can be found on this page.
Substance Abuse (2024 changing to Substance Use and Addiction Journal)
- "Non-Pejorative Language - SAj supports the mission AMERSA which is “to improve health and well-being through interdisciplinary leadership in substance use education, research, clinical care, and policy.” The SAj Editorial Team believes that improving health and well-being requires interdisciplinary leadership regarding the language that we use in our scholarship. We ask authors, reviewers, and readers to carefully and intentionally consider the language used to describe alcohol and other drug use and disorders, the individuals affected by these conditions, and their related behaviours, comorbidities, treatment, and recovery in our publication. Specifically, we make an appeal for the use of language that:
- Respects the worth and dignity of all persons (“people-first language”)
- Focuses on the medical nature of substance use disorders and treatment
- Promotes the recovery process
- Avoids perpetuating negative stereotype biases using slang and idioms
- Strongly recommends the use of “people-first language”
- Authors should use inclusive and person-first language in manuscripts. Describe people as having a condition or disease, experiencing a circumstance or doing something specific rather than the condition, disease, circumstance or activity being part of their identity. For example, use “people with obesity,” “person with HIV,” “person who injects drugs,” “people experiencing homelessness,” etc.
- Strongly recommends the use of “people-first language”
Person/People First Language - Recommendations, Guidelines, Commitments
PFL - Smoking, Tobacco, Nicotine
American Psychiatric Nurses Association: POSITION STATEMENT: Psychiatric-Mental Health Nursing’s Role in Tobacco Treatment
- "Smoking and tobacco use are widely recognized as an addiction, not merely a personal choice, and health care clinicians increasingly address this chronic, relapsing disease using recovery-oriented language. Terms such as “cessation” are being replaced with “treatment” and “smoker” replaced with person-first language such as “person who smokes.”
Anesthesia Experts - Person-First Language in Anesthesiology Care
- So, is person-first language objectively superior to nonperson-first language? An increasing body of research suggests that it is. Many of the diseases and conditions frequently used to stand in for a person with the condition are those in which there is an unstated or even explicit implication that lifestyle choices are responsible for the condition (alcoholic, addict, diabetic, cirrhotic) or otherwise telegraph shame directed at the patient with the diagnosis (obese, epileptic, smoker). Using person-first language promotes respect and dignity for patients. Describing someone as “a patient with diabetes” rather than “a diabetic” acknowledges that the person is more than just their illness and recognizes their individuality. Using person-first language also helps to avoid stigmatization and discrimination, which can have a negative impact on a patient’s mental and physical well-being (Diabetes Spectr 2018;31:58-64). This may be especially true for mental health conditions, substance use disorders, painful syndromes, eating or body image-related conditions, and in obstetric care (Int J Drug Policy 2010;21:202-7).
CDC - Centers for Disease Control and Prevention: Preferred Terms for Select Population Groups & Communities
- Instead of this… "Smokers," Try this... "People who smoke"
Change Lab Solutions - Justice In The Air: Framing Tobacco-Related Health Disparities A FrameWorks Strategic Brief
- Use person-first language. Avoid labeling people as “smokers” or “tobacco users.” Instead, start with people, then add any necessary qualifiers: people who smoke, people with a dependence on nicotine.
- Use tobacco use disorder instead of smoker.
- Person-first language can reduce stigma – a patient “has” rather than “is” a condition
- Avoids negative bias, punitive attitudes, and blame
- The NCSCT has committed to using ‘people first’ language wherever possible, so instead of ‘smoker’ we will talk about ‘people who smoke’ or just ‘people’
- NICE style guide (downloadable document)
- Smoker: Do not use. In line with our house style, we do not label people. Use 'people who smoke'. [emphasis added]
- Don't label people with their condition: we would never say 'epileptics', 'schizophrenics', 'smokers', 'drug-takers'. Use the following as a guide: 'people with epilepsy', 'people with schizophrenia', 'people who smoke', 'people who take drugs'.
- Use person-first language (“person who smokes” not “smoker”).
- Instead of: smoker (e.g., patient is a smoker)
- Use: smokes (e.g., patient smokes cigarettes)
- STR’S COMMITMENT TO NON-STIGMATIZING LANGUAGE IN LUNG CANCER CARE
- "Whether we as chest imagers realize it or not, our very language can have a negative impact on the care for the patients we serve. As published studies continue to demonstrate, smoking-related language bias often stigmatizes our patients with a smoking history and results in suboptimal care and less than desirable clinical outcomes... Instead of a report stigmatizing the patient as a “smoker,” consider describing the patient as a “person who smokes.” Rather than a “nicotine addict,” an expression such as a “person with a nicotine dependence” attenuates the common stigmatization of these patients. One will notice these alternative descriptors utilize a person-first approach rather than a habit-based one. This approach can and should be adopted in publications, society and conference presentations as well as in daily training with residents and fellows. Ultimately, this language shift more precisely aligns itself with a core underpinning of our approach to care – respect for our patients.
Truth Initiative's Ex Program - How to Reduce Mental Health Stigma, Smoking Stigma in the Workplace
- It can be tempting to dismiss these kinds of negative labels as simply semantics, but research has shown that language matters. Using person-first language like “people who smoke” instead of “smokers” acknowledges the tenacity of this disease, conveys dignity and greater respect, and can reduce smoking-related stigma.
University of Melbourne - Melbourne School of Population and Global Health
- All communications materials aimed toward potential and enrolled LCS participants must be created sensitively and incorporate the plain English guidelines to be accessible to those with low levels of health literacy. This includes clear, short sentences that use active verbs. It is also important to avoid stigmatizing language, as this can affect the care provided to patients, impact the attitude of other health care providers towards the patient, and can adversely impact health outcomes. Therefore, language used within such materials – from promotion materials to results letters – must aim to reduce the burden of stigma already experienced by these high-risk populations.
- As part of a communications strategy, the International Association of Lung Cancer (IALSC) Language Guide should be adopted across all communications tools and resources and be included as part of HCP education and training.
- IASLC’s four simple principles:
- Use person-first language. For example, instead of “lung cancer patient” use “patient/person with lung cancer.”
- Eliminate blaming language. For example, replace “patient failed treatment” with “treatment failed patient.”
- End stigma. For example, instead of “smoker” use “person who smokes.”
- Equity. Follow best practices regarding race, ethnicity, gender, socioeconomic, and geographic descriptions to promote cultural humility and sensitivity.
- IASLC’s four simple principles:
PFL - Not Tobacco
ADA National Network - Guidelines for Writing About People With Disabilities
- In general, refer to the person first and the disability second. People with disabilities are, first and foremost, people. Labeling a person equates the person with a condition and can be disrespectful and dehumanizing. A person isn’t a disability, condition or diagnosis; a person has a disability, condition or diagnosis. This is called Person-First Language.
- However, always ask to find out an individual’s language preferences. People with disabilities have different preferences when referring to their disability. Some people see their disability as an essential part of who they are and prefer to be identified with their disability first – this is called Identity-First Language. Others prefer Person-First Language. Examples of Identity-First Language include identifying someone as a deaf person instead of a person who is deaf, or an autistic person instead of a person with autism.
- Recommends person-first language.
- "Compiled by INPUD and the Asian Network of People who Use Drugs (ANPUD), this guide aims to explain our current position on the use of language and to provide clear advice on what is acceptable to us as communities of people who use drugs. We want to encourage all people to be thoughtful about the language and words they use, and have therefore provided a reference guide that identifies stigmatising language and gives non-judgemental, strengths-based, and respectful alternatives."
Massachusetts Down Syndrome Congress - People First Language
- As part of the disabilities rights movement, MDSC promotes the use “People First language” because people with disabilities are NOT their diagnoses or disabilities. They are PEOPLE first. MDSC is not only committed to using People First language in all materials, statements, and interactions. We also work to educate and encourage the community at large to do the same.
Minnesota Organization for Habilitation and Rehabilitation - MOHR supports People First Language
- Although a disability has an impact, it is only a small part of a person’s identity. No one is their disability. We encourage you to see people with disabilities as people, first. Using the “People First” language we describe is one way to let people know you see them, not just their disability. When you see people first, you and they will notice the difference.
- The Narcolepsy Charter champions the right for people with narcolepsy “to live in a society that understands and recognises the impact of narcolepsy” and encourages “the ability to talk about narcolepsy without fear or judgement”. Given that referring to “narcoleptics” rather than “people with narcolepsy” is very likely to perpetuate unhelpful stereotypes and negative attitudes, Narcolepsy UK encourages people with and without narcolepsy to put people first and avoid the term “narcoleptics” or “narcolepsy patients” in favour of “people with narcolepsy”.
United Nations Office at Geneva - DISABILITY-INCLUSIVE LANGUAGE GUIDELINES
- This document contains recommendations that United Nations staff, experts and collaborators can use in their oral and written communications on disability or other subjects, including speeches and presentations, press releases, social media posts, internal communications and other formal and informal documents.
- People-first language is the most widely accepted language for referring to persons with disabilities. It is also the language used in the Convention on the Rights of Persons with Disabilities. People-first language emphasizes the person, not the disability, by placing a reference to the person or group before the reference to the disability. For example, we can use expressions such as “children with albinism”, “students with dyslexia”, “women with intellectual disabilities” and, of course, “persons with disabilities”.
- However, the people-first rule does not necessarily apply to all types of disabilities. There are some exceptions. (Deaf, Blind, Autistic)
Publication Policies - Language (General)
- Twitter(X) Thread by Lead Author
- Editors, reviewers, authors and readers of Addiction agree that journal articles should not contain terminology that harms vulnerable groups, but disagree about which terms those are and what should replace them. Addiction therefore promotes principled, civil discussion when such disagreements occur.
- PRINCIPLE 1: EVERYONE IS ALLOWED TO REFER TO THEMSELVES AS THEY WISH
- PRINCIPLE 2: WHETHER A POPULATION WANTS TO BE CALLED A PARTICULAR TERM IS AN EMPIRICAL QUESTION
- PRINCIPLE 3: WHETHER ANY PARTICULAR TERM IS HARMFUL IS AN EMPIRICAL QUESTION
- PRINCIPLE 4: HISTORICAL ACCURACY IS A SCHOLARLY OBLIGATION
- Article: The Burden of Proof Is on the Language Police
Speaker/Presenter Policies
- We are proud to support and officially endorse the People First Charter! Language matters - the use of positive and inclusive language is a vital tool in tackling stigma and discrimination. Person-first language simply puts people before their condition, recognizing that people are people, and are not defined by their condition. In HIV care, we should avoid terms like 'HIV-infected people' and use 'people living with HIV'. As a participant, faculty member, or abstract presenter at one of our programs, we encourage you to consult these guidelines as you prepare program-related materials.
- When preparing an abstract, remember that ACPA requires that all abstracts use person first language, e.g., instead of “cleft patient” use “patient with a cleft.”
- ‘PEOPLE FIRST’ language is required for the abstracts (e.g. person with alcohol use disorder instead of ‘alcoholic’). Examples of appropriate terminology are provided in the editorial in Substance Abuse, cited below, and accessible at https://pubmed.ncbi.nlm.nih.gov/24911031/
- Broyles, L.M., Binswanger, I.A., Jenkins, J.A., Finnell, D.S., Faseru, B., Cavaiola, A., Pugatch, M. & Gordon, A.J. (2014). Confronting inadvertent stigma and pejorative language in addiction scholarship: A recognition and response. Substance Abuse, 35(3), 217221.
- American Physical Therapy Association - Pennsylvania
- 5. Professional Presentation/Quality
- a. Adherence to formatting requirements evident.
- b. Abstract clearly and concisely written.
- c. Use of correct spelling and proper grammar.
- d. Use of people first and inclusive language.
- Oral Abstract Presentation Guidelines... Use people-first language: We encourage presenters to use people-first language when referring to individuals. This means describing individuals as people with a medical condition rather than focusing on their diseases or disabilities. This promotes inclusivity and respect.
- It is important to use “people first” language such as “people with HIV” rather than “HIV-infected people.” Similarly, do not characterize people by their conditions. “People with diabetes” is preferred over “diabetics”; “patients with cirrhosis” rather than “cirrhotics;” and “people who inject drugs” rather than “drug abusers.” Out of respect for their contributions to our scientific advances, avoid calling study volunteers “subjects.” The preferred terms are study “participants” or “volunteers.”
- We strongly encourage anyone who submits an abstract or clinical case to use people first language.
- Please ensure that you refer to the EASO Person First Language Guide when preparing your abstract AND developing your presentation. Please note that abstracts that do not use Person First Language will be rejected.
- Abstract submitters are strongly encouraged to use person-first language in their abstracts.
- The Guide is not long, dense, or difficult to understand. It encourages everyone to “take conscious steps to be thoughtful in the language we use,” and boils down to four simple, subtle principles:
- Use Person-First Language: For example, instead of “lung cancer patient,” use “patient/person with lung cancer.”
- Eliminate Blaming Language: For example, replace “patient failed treatment” with “treatment failed patient.”
- End Stigma: For example, instead of “smoker,” use “person who smokes.”
- Equity: Follow best practices regarding race, ethnicity, gender, socioeconomic, and geographic descriptions to promote cultural humility and sensitivity.
- “We came together from different places, with different methods and different training, but we all agree that words matter, and that it is possible to change the language we use to talk to and about persons with lung cancer, as well as about people who use tobacco,” Dr. Ostroff said. “And we can do that in a way that that conveys respect, inclusivity, and equity.”
- Follow-up on new policy: 2024: Preprint: Brief Report: Precision Language and Deletion of the “S” Word 2022
- "In 2021 the International Association for the Study of Lung Cancer (IASLC) published the IASLC Language Guide as guidance on preferred language and phrasing in oral and written communications, including presentations at conferences. This study analyzed presentations from the 2022 IASLC World Conference on Lung Cancer (WCLC) one year after implementation of the Language Guide to identify adoption rates of non-stigmatizing language and to determine correlations with presenter characteristics."
- We searched each presentation, including images, for discussion of tobacco use, and the use of the term “smoker,” which is an indicator of stigmatizing language.
- Of 177 presentations that discussed smoking status 77 presenters used non-stigmatizing language while 100 presenters used the stigmatizing term "smoker". Male MDs and female PhDs and non-medicine subspecialties and advocates were more likely to use non-stigmatizing language.
- Encouragingly, only after one year post release of the Language Guide, greater than one-third of the presenters at the WCLC used non-stigmatizing language. This finding represents a step towards improving respectful and inclusive language surrounding smoking within the thoracic oncology community.
- As you prepare for your presentation at NUTRITION 2023, ASN strongly recommends that presenters use people-first language. This includes describing individuals as people with a medical condition rather than as diseases or disabilities. Terms such as “adults with obesity” and “children with diabetes” are preferred over “obese adults” and “diabetic children”. For more information consult “Use of people-first language with regard to obesity” Am J Clin Nutr 2018;108:201 or “The Effect of Words on Health and Diabetes” Diabetes Spectrum 2017;30:11- 16.
- PEOPLE FIRST LANGUAGE: The Obesity Society requires use of person-first language and nonstigmatizing images in all written and verbal communications. For more information please visit: https://obesityweek.org/abstracts/speaker-resources/person-first/.
- Please use People-First Language in your abstracts and presentations to respectfully refer to individuals with chronic conditions and disabilities. This language refers to the person first, not the condition or disability. It serves to eliminate bias, labels, stigma, and discrimination. Some examples: “children with obesity” instead of “obese children,” or a “child with a developmental delay” instead of a “developmentally delayed child.”
- The use of People-First Language is mandatory for the abstract to be accepted. Abstracts not using People-First Language will be rejected.
Guidelines - Journalists and Editors
- While this guide does not mention smoking or nicotine, it provides helpful suggestions on ways to avoid stigma when writing about the use of substances, that are applicable to smoking and nicotine.
Videos
2024: Breathe Easy Maine Webinar Addressing the Harmful Effects of Tobacco-Related Stigma
- Presenter: Derek Bowen, MaineHealth Center for Tobacco Independence
- Stigma is the public’s effect of marking disgrace of a certain quality within a targeted community. People who use tobacco are faced with stigma and the challenges it brings day by day, and it leaves a great impact on the individual’s quality of life, mental health, and likeliness to stop using tobacco further down the road. Within the webinar, we will discuss different types of stigmas, the effects of stigma, and ways to reduce and prevent stigma when it comes to individuals who use tobacco.
2021: E-Cigarette Summit: Stigma and tobacco harm reduction: what we can learn from other health behaviors
- Prof Scott Leischow
- Stigmatizing smoking has been at the heart of tobacco control efforts for decades, which may drive more people to quit but at the same time potentially create new difficulties for smokers, including self-isolation, creation of social groups that might become ‘hardened’ to changing smoking behaviors, and perceptions by the user and society that complete abstinence is the only option. The stigma associated with a wide variety of behaviors has impeded progress toward improving population health in some cases, such as the reticence in making products and services available that could reduce the risk of communicable disease (eg needle exchanges), as well as harm reduction products that could benefit users and society when an individual addicted to a substance is not able to or chooses not to become completely abstinent (eg NRT, ENDS, smokeless tobacco). This presentation will explore some of the conflicting aspects of stigma in tobacco control, explore similarities and differences regarding the stigma of using of different addicting substances, and consider some research, practice and policy directions.
2017: Video: Sarah Jakes
- Ecig Summit UK
- How are you doing? How are you really doing?
Studies, Papers, Reports - Smoker
- The public should be educated about the difficulties in exercising self-control in addictions, such as nicotine addiction, and other lifestyle-related afflictions, such as obesity, so that moralization and its social consequences are less likely to occur. Such cognitively-oriented initiatives should be accompanied by emotionally oriented ones, aiming to sensitize the public to the moralized groups’ suffering.
- Changes in our language can convey a less stigmatizing description of individuals (eg, person who smokes instead of “smoker”).
- To balance these factors, complementary campaigns can address the role of media and the tobacco industry in promoting smoking, making it clear that smoking is not solely driven by personal decision making, emphasize that smoking is a physical and behavioral addiction and not a personal moral failing, use person-first language (people who smoke vs. smokers), emphasize the positive benefits of quitting, and acknowledge that quitting is difficult and may take multiple tries but there are treatment strategies that can help. [emphasis added]
- However, the descriptors we commonly use to classify people who smoke may inadvertently perpetuate harmful, stigmatizing beliefs and negative stereotypes. In recognizing the power of words to either perpetuate or reduce stigma, Dr. Nora Volkow—Director of the National Institute on Drug Abuse—recently highlighted the role of stigma in addiction, and the movement encouraging the use of person-first language and eliminating the use of slang and idioms when describing addiction and the people whom it affects.
- In this commentary, we make an appeal for researchers and clinicians to use person-first language (eg, “people who smoke”) rather than commonly used labels (eg, “smokers”) in written (eg, in scholarly reports) and verbal communication (eg, clinical case presentations) to promote greater respect and convey dignity for people who smoke. We assert that the use of precise and bias-free language to describe people who smoke has the potential to reduce smoking-related stigma and may enhance the precision of scientific communication. [emphasis added]
- "Indeed, an oft-spoken proverb among those who work in tobacco control is “There is no such thing as a ‘smoker,’ there are only people who smoke." This framing intentionally creates space to decouple behavior from identity, so that unhealthy behavior (i.e., smoking) can be actively denormalized without perpetuating stigma against those who engage in it. It underscores that individuals who smoke maintain their core humanity and value as human beings, despite engaging in a socially unacceptable behavior. Once they change this target behavior, they are no longer targeted for disapproval." [emphasis added]
- Stigmatizing language can worsen addiction-related stigma and outcomes. Although non-professional terminology may be used by individuals with addiction, the role of clinicians, educators, researchers, policymakers, and community and cultural leaders is to actively work toward destigmatization of addiction and its treatment, in part through the use of non-stigmatizing language.
- Stigmatizing Language: Smoker
- Proposed Terminology: Person with cannabis and/or tobacco or nicotine use disorder, or addiction involving cannabis / tobacco / nicotine use.
- Related Article: Shaming Smokers Actually Increases Their Urge to Light Up
- In a study, smokers who were confronted with negative stereotypes commonly associated with smoking were more compelled to light up sooner than smokers who weren’t thusly goaded.
- For the purposes of this manuscript, we have attempted to reduce the stigma associated with smoking and support a more holistic approach by referring to “individuals who smoke” or “patients who smoke” rather than referring to people as “smokers.” In other words, tobacco dependence is just one component of an individual’s health behaviors and diagnoses. [emphasis added]
- "For these reasons, the Editorial Team of Substance Abuse seeks to formally operationalize respect for personhood in our mission, our public relations, and our instructions to authors. To our knowledge, few journals have explicitly taken this step,7–12 and we are the first scientific addiction journal to do so. Our overarching call is threefold. First, we are asking authors to carefully and intentionally consider the language they use to describe alcohol and other drug use and disorders, the individuals affected by these conditions, and their related behaviors, comorbidities, treatment, and recovery..."
- Appendix C. Comments on antcipated changes to practce: 'people who smoke' not 'smoker' [emphasis added]
- Sci-Hub (full paper)
- I use the terms “tobacco user” and “people who smoke” to counter the pejorative implications of the term “smoker(s)”
- I found that most of the tobacco and health advocates I encountered held dismissive and demeaning views about people who smoke...
- The themes identified illustrated how nonsmokers’ perception of smoking as illogical and self-destructive supported harsh reactions, including stigmatizing behaviors that antagonized smokers.
- A supportive/empathic tobacco-control denormalization approach could enhance young adult smokers’ willingness to make the transition from smoker to smoke free and elicit stronger support for their efforts from nonsmokers.
Editorials, Articles, Websites, Blogs - Smoker (Some from Journals)
2025: Nicotine and Tobacco Research: Editorial: Person-First Language in Nicotine and Tobacco Research
- Click on "PDF" to read the editorial
- "Embracing person-first language is a crucial step toward scientific precision in language use, and will help to achieve an equitable and respectful approach to research on nicotine and tobacco use. By prioritising the individual over their behaviour, we as a research community can foster a culture of linguistic accuracy and precision, which also demonstrates empathy and understanding towards those who use nicotine or tobacco containing products."
2024: International Journal of Drug Policy: Editorial: Guiding principles for breaking down drug-related stigma in academic writing
- “…although stigma relating to alcohol, tobacco and prescription medicines is increasingly well documented…This stigmatisation is produced through words like “criminal”, “abuser”, “junkie”, “alcoholic”, "smoker" and “addict”. These kinds of words have functioned in tandem with corresponding normative reactions such as fear and disgust, to justify and legitimise stereotyping, discrimination, punishment, social control and exclusion, and create significant obstacles to treatment, harm reduction, support, health and wellbeing.”
2023: The Lancet Oncology: Editorial: Patient first; person first
- "Dehumanising and stigma-laden terminology is rife in medicine, with oncology being no exception, and blame-ridden language is too often used when referring to people at risk for or who have cancer. Although not coming from a place of malice, or indeed reflective of an intentional effort to offend, these phrases are typically used as shorthand in an effort to aid communication, but the lack of empathy and awareness that accompanies the use of such language could also be linked with apathetic attitudes."
- "Presenters at the conference promoted the benefits of implementing the IASLC Language Guide, which emphasises the importance of using person-first language (eg, using patient or participant rather than subject, and person with active tobacco use rather than smoker), eliminating blame language (using unable to comply rather than non-compliant), and ending stigma (such as noting a person who does not smoke rather than a non-smoker)."
2023: Filter: Article: Is It Time to Abandon the Term “Smoker”?
- It’s exactly that stigma that society has attached to the word—leaving little room for nuance or reinvention in the fixed, judgemental glare of a label—that’s prompting growing numbers to move away from its use.
2023: FINN Partners: Blog: Watch Your Language: Words Matter in Scientific and Health Communications
- "While some language conventions have stagnated, others have started to move in more positive directions. For example, terms such as “diabetic” or “smoker” are being replaced with “a person living with diabetes” and “a person who uses cigarettes.” While the former terms were always clearly understood, they had the effect of defining the individuals as their disease or risk factor. The latter terms acknowledge the person first."
2022: Nicotine & Tobacco Research: Editorial: Time to Stop Using the Word “Smoker”: Reflecting on the Role of Language in Advancing the Field of Nicotine and Tobacco Research
- From legislatures to schools to workplaces, as well as in scientific discourse and clinical practice, the past few decades have seen a move away from labels such as “user,” “addict,” or “alcoholic,” for their lack of precision, negative connotation, and the way they equate the person with behavior or condition. Despite this, “smoker” remains in use in tobacco research, as well as in clinical settings and public health policy.
2022: John Oyston: Blog: PWS – People Who Smoke
- The word “smoker” is a disparaging term, like “addict” or “alcoholic”
- The use of a label such as “smoker”, “addict” or “illegal” divides people up into “us” and “them”. It is a slippery slope toward calling certain groups or tribes “vermin” or “cockroaches”
2022: EX Program by Truth Initiative: Blog: How to Reduce Mental Health Stigma, Smoking Stigma in the Workplace
- It can be tempting to dismiss these kinds of negative labels as simply semantics, but research has shown that language matters. Using person-first language like “people who smoke” instead of “smokers” acknowledges the tenacity of this disease, conveys dignity and greater respect, and can reduce smoking-related stigma.
- People who smoke are often perceived as having negative personality and social traits.
- These aren’t silent biases either: these negative perceptions influence attitudes about people who smoke, which in turn influence non-smokers’ willingness to interact with people who smoke.
- ...there are 21 states that do not offer employment protection to tobacco users, allowing employers to refuse to hire people who smoke. Unsurprisingly, people who smoke have a harder time getting hired. For example, the chances of getting a job within a year is reduced by 24% for unemployed job seekers who smoke compared to non-smokers, even when other factors like criminal history are considered.
- And even with a job, the stigma still carries through, as people who smoke earn 20% less compared to non-smokers.
- Stigma associated with many mental health conditions like depression is now a well-recognized issue. By acknowledging this stigma, it has allowed considerable progress to be made. Unfortunately, the same progress has not been made in reducing the stigma of substance use disorders like nicotine addiction.
2021: ECOG-ACRIN Cancer Research Group: Blog: A New Guide Encourages the Use of Language that is Respectful of Patients, Free of Stigma, Inclusive, and Equitable
- End stigma: Promote judgment-free, bias-free language. Try 'person who smokes' rather than 'smoker.' [emphasis added]
- 'A person with nicotine dependence' instead of 'a nicotine addict.'
- "Smoking and tobacco use are widely recognized as an addiction, not merely a personal choice, and health care clinicians increasingly address this chronic, relapsing disease using recovery-oriented language. Terms such as “cessation” are being replaced with “treatment” and “smoker” replaced with person-first language such as “person who smokes.”"
- Link on WayBack Machine
2019: Filter: Article: Widespread Anti-Smoker Stigma Is Harmful, as Well as Wrong
- "Ordinarily, stigmatizing a disease or observing medical practitioners making decisions based on social characteristics would raise the hackles of the public health community. With smoking, however, this hasn’t been the case. In fact, many anti-smoking campaigns actually turn to stigmatization as a behavioral control tactic."
Comments by people who don't smoke
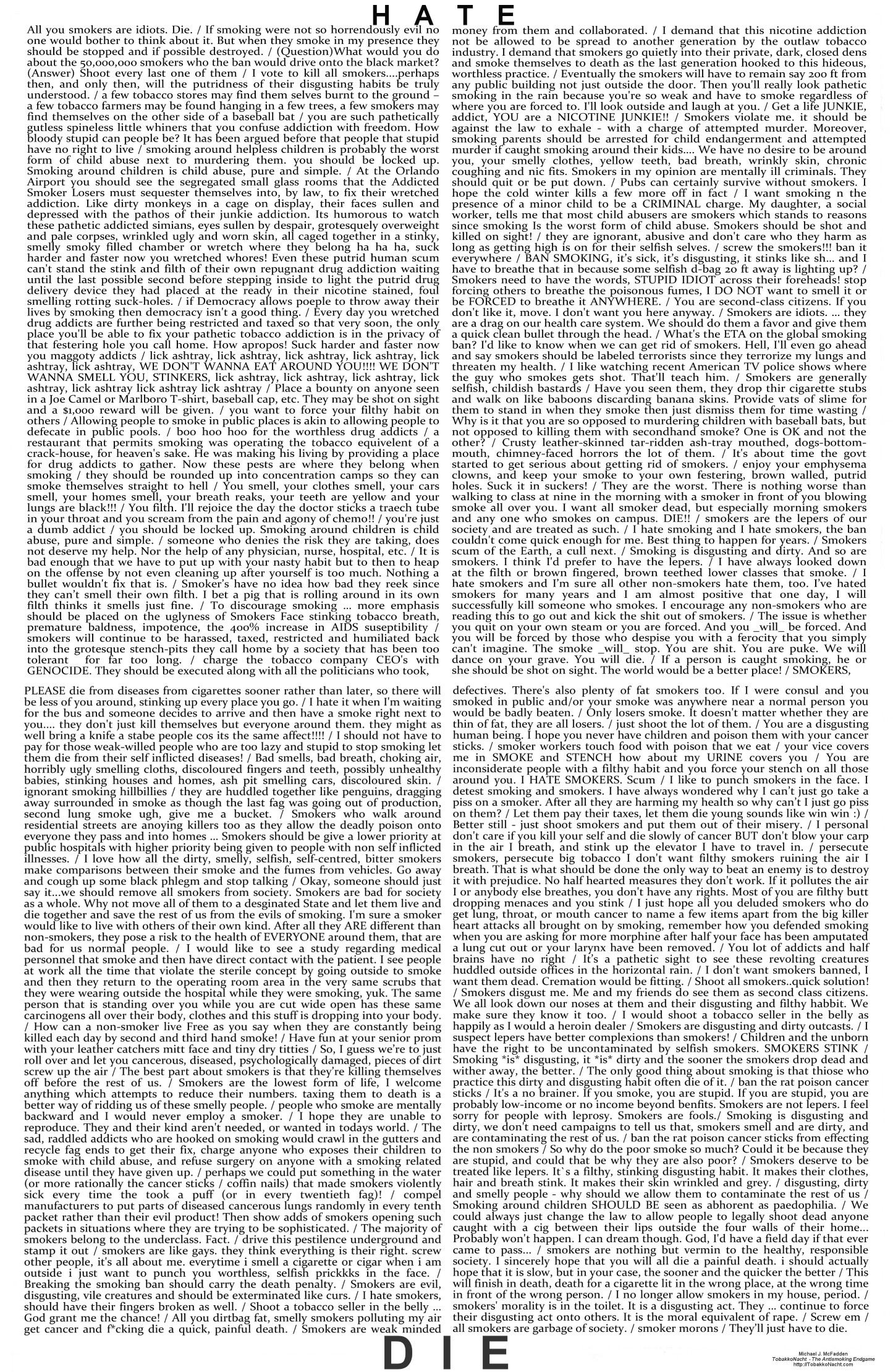
- 2021: The Wall of Hate
- 130 comments found online. Some of those comments suggest violence against people who smoke
- Wall of hate info
- 2014: Let's Not Wage War on Smokers
- In 2006, sociologist Hannah Farrimond and psychologist Helene Joffe asked 40 British adults what they thought about smokers. It wasn’t nice. Non-smokers use terms such as ‘outcast’, ‘persecuted’, ‘lepers’, ‘under-class’ and ‘blacklisted’ to describe smokers’ status in society….Non-smoking participants associate smokers with a strong negative aesthetic. This comprises two aspects, smell (e.g. ‘reek’, ‘pong’, ‘stink’, ‘stale’, ‘old’) and negative appearance (‘stained yellow fingers’, ‘grey, dry, wrinkly skin’, ‘brown teeth’)…several non-smokers see smokers as lacking in cleanliness and engaging in poor self-care.
{kind=link}
- Drs. Carter-Harris and Williamson both encourage people to use person-first language when talking about smoking. One example of this is describing someone as “a person who formerly smoked” rather than “a former smoker.”
- “By labeling someone as a smoker, you’ve depersonalized them, and you’ve identified them by a behavior that’s stigmatized,” Dr. Carter-Harris said.
- "Remember that poor woman who ignited her oxygen tube with a lighter? Seek it out – look at the comments and see what the public thinks of smokers. The vitriol and hatred is something to behold. A poor woman made a horrible mistake whilst still under the effects of a general anaesthetic and what did the public say? She deserved it. Why? Because she was a smoker."
- In 2004, a team of health scientists at Oxford interviewed 45 people with lung cancer and found that felt even more stigma than other cancer patients: Participants experienced stigma commonly felt by patients with other types of cancer, but, whether they smoked or not, they felt particularly stigmatized because the disease is so strongly associated with smoking… Some patients concealed their illness, which sometimes had adverse financial consequences or made it hard for them to gain support from other people.
Tweets about discontinuing the use of "Smoker," or using person-first language
- I encourage authors who submit to Harm Reduction Journal Tobacco Section to use person-centred language. People are not defined by 1 behaviour they do.
- I write “people who smoke/have smoked.” I haven’t read any research on this particular term, but referring to “smokers” in journalistic articles never sat well w me bc it reduces people’s identity to a single activity that may be one they’ve tried to quit.
- What would it take for me to convince the scientific and public health communities to switch from the stigmatizing word "smokers" and switch to something else? Perhaps "people who smoke (PWS)."
- You're 100% correct - admittedly, when on autopilot, I've written "smokers" and revised when editing. I'm a fallible human, a work in progress, and trying to do better. What would it take? keep calling us out on it! we need to retrain our brains.
- This is right & we’ve had a lot of conversations about this at TC_BMJ but I know some still slip through. Anyway, the point is our concern ought to focus on these horrible products, not on individual behaviors. Thank you for this reminder.
- When reviewing articles that use the word "smoker" or something similar, I suggest to the authors to use person-centered language and then write a nice note to the editor encouraging wiggle room with the word limit
- Reply by Benjamin Toll: This is a great thread! I also want to alert everyone to Jamie Ostroff's great article on same topic: https://ncbi.nlm.nih.gov/pmc/articles/PMC7733058/ I am thrilled to see @MaloneRuth considering for @TC_BMJ & I hope you are addressing word limits? It is the major hurdle for me with papers and grants
- Reply by Larry Hawk: Old habits are hard to break, but we are behavior change specialists. I'm committed to change and will roll with the occasional slips/relapses. PWS, not smokers. PWS, not smokers...
- Hearing "smoker" a lot....at @healthvermont we prefer "person who uses tobacco" or "tobacco user" to remove the stigma, and use people-first language.
- New paper - Centering authors' responsibility to engage w/ people who use drugs & respect their preferences, we argue using people-first strengths-based & inclusive language with care breaks down #DrugStigma & builds equitable values policies & practices
- Subject near and dear to my heart …. People in every area of drug research would benefit from reading, but particularly those in tobacco control and tobacco industry. None of us are off the hook.
Examples: People Who Smoke
- "People who smoke" are mentioned 16 times in this report. One example: "These particular examples also shine a light on the potential of e-cigarettes for people who smoke and live in social housing. Reviews of the evidence by the National Academies of Sciences, Engineering and Medicines in the US and the UK Committee on Toxicity have concluded that the relative risk of adverse health effects from e-cigarettes are likely to be substantially lower than from smoking. E-cigarettes have also been shown to be an effective aid for quitting, in clinical trials and at population level, with some evidence suggesting they are even more effective than traditional forms of nicotine replacement therapy, like patches and gum. They also appear to have been particularly valuable among groups who face higher levels of addiction and more barriers to quitting, for example among people experiencing homelessness and people with mental health conditions. Considered alongside the evidence from the ‘Swap to-Stop scheme, e-cigarettes therefore present a real opportunity to substantially benefit people who smoke and live in social housing."
- "Today, to mark World No Tobacco Day, the Honourable Patty Hajdu, Minister of Health, announced $3 million in funding for a national social marketing campaign to encourage people who smoke to quit."
- "Some people who smoke choose to try e-cigarettes to help them stop smoking. Stopping smoking clearly has well-documented health benefits...People who have already switched completely from smoking to e-cigarettes should not switch back to smoking (either solely or along with e-cigarettes), which could expose them to potentially devastating health effects."
Studies, Papers, Reports - Smoking (Stigma)
- "Tobacco denormalisation deliberately encourages beliefs that people who smoke are selfish, unattractive, ‘addicts’, of ‘lower class.'" "Critics argue that this approach to tobacco denormalisation is discriminatory, stigmatises people who smoke, and may prevent smokers from seeking help to quit or be treated for tobacco-related diseases."
- "There is little evidence that the BDMA [brain disease model of addiction] has reduced the stigma suffered by people who smoke cigarettes." "Indeed, in many studies, people who smoke report experiencing significant stigma. Stigma has also arguably increased as cigarette smoking has become concentrated in the least educated and most socially disadvantaged groups in the populations of high-income countries."
- "In principle, public acceptance of a BDMA for smoking could have produced a more sympathetic response to people who smoke cigarettes, but survey evidence suggests that this has not happened. On the contrary, as population smoking prevalence has declined, the stigmatisation of smokers seems to have increased because smoking is concentrated among the most disadvantaged members of the population. Furthermore, the strategy of labelling people who smoke as “addicts” may increase the association between smoking and a spoiled identity. In principle, the BDMA could support policies that promote the use of less harmful forms of nicotine delivery to people who are unwilling or unable to quit smoking. In practice, however, it seems more likely to be used to justify bans on the sale of products that deliver nicotine in less harmful ways than combustible cigarettes, because these products can produce addiction."
- Frohlich et al and others have suggested that public health educational messages may have the unintended consequence of marginalizing low-income smokers and unintentionally contributing to health disparities. Our study participants also point to healthcare professionals as an important group who may be contributing to these feelings. With this in mind, efforts to educate healthcare providers on how their actions may be perceived as judgmental or lacking in compassion about the effects of nicotine withdrawal are warranted.
- However, smoking prevalence remains disproportionally high in socioeconomically disadvantaged groups.
- Smoking stigma, particularly self-stigma, underpinned accounts, with two overarching themes: interplaying barriers and enablers for creation of a smoke-free home...
- Personal motivation to abstain or stop smoking empowered participants to reduce or quit smoking to resist stigma. For those struggling to believe in their ability to stop smoking, stigma led to negative self-labelling.
- Whilst denormalisation of smoking has been a useful public health tool for reducing smoking rates in the UK, it is arguable that this can lead to unhelpful stigmatisation of already vulnerable disadvantaged groups.
- The stigma reduces the funding available for lung cancer research. In the US, federal funding for lung cancer research per lung cancer death is only 15% of the funding amount for breast cancer per breast cancer death.
- In a Global Lung Cancer Coalition survey, one in five people (21%) agreed with the statement that they have less sympathy for people with lung cancer than for people with other types of cancer.
- Stigmatization of smokers has the greatest impact on the socioeconomically deprived, the disadvantaged populations. These populations have the highest prevalence of smokers and encounter the stigma of their race or disadvantage (poverty, disability, sexual preference, behavioral health etc.) in addition to the stigma associated with smoking.
- This stigmatization leads people who smoke to be less likely to seek medical care when they have symptoms, more likely to lie about their smoking, more likely to be refused access to care including curative surgery for early stage lung cancer unless they quit smoking, less likely to be offered smoking cessation help if they are uncomfortable disclosing their smoking status due to stigma and bias from their healthcare professional.
- "Thus, stigmatization led smokers toward emotional, cognitive, and attitudinal reactions that might make them less likely to quit."
- This study suggests that perceived smoking-related stigma may be associated with more quit attempts, but less successful quitting among smokers. It is possible that once stigma is internalized by smokers, it may function as a damaging force.
- Consistent with previous research we have found that smokers’ who reported greater feelings of stigmatization about their smoking were more likely to report having made recent quit attempts and report a stronger intention quit smoking in the future.
- It is also important to recognize the potential negative consequences associated with stigmatizing smokers, who may seek ways to evade stigma by segregating themselves into groups accepting of smoking and perhaps fostering the development of fatalistic attitudes about their ability to change their smoking behavior, which make quitting smoking harder to accomplish. Thus, behavioral interventions for smoking cessation might include addressing stigma-related issues as part of the quitting process.
- In addition to the health disparities experienced by smokers, psychosocial factors such as smoking stigma can cause additional strain on health, and may thwart positive behavior change. Smoking stigma can be defined as a social process by which exclusion, rejection, blame or devaluation occurs,7 in this case related to smoking or being identified as a smoker. Stigma can be categorized as: 1) internally-focused self-stigma resulting from the internalization of public stigma and characterized by statements about the individual's worth, e.g., “I am worth less because I smoke”; 2) perceived or felt stigma, which is an awareness of devaluation or stereotype in work, social, and everyday situations, and includes fear of being stigmatized, experiencing external blame, and social isolation; or 3) enacted stigma, which refers to acts of discrimination perpetrated on stigmatized individuals.
- We would consider, however, efforts to induce stigma as abjectly wrong and avoidable. Instead, treatment engagement strategies could emphasize stigma-reduction as an ancillary benefit – i.e., messaging that quitting smoking can reduce stigma, rather than messaging aimed at increasing stigma to induce quitting.
- However, continued smoking was also a source of negative emotion, as women felt shame, guilt and low self-esteem over their inability to quit, which was perceived by some as indicative of weakness. These negative self-perceptions are consistent with stigmatized views of smokers held by the public. Women also expressed feelings of defiance about their smoking despite pressure to quit and identified external factors which contributed to their inability to quit. The negative emotions, self-stigma and shame experienced by low income American Indian and African American women smokers may contribute to continued smoking and disrupt quit attempts. Additional research is needed in order to develop effective tobacco cessation interventions for this group.
2009: The Psychological Effects of Social Stigma: Applications to People with an Acquired Hearing Loss
- To various extents, people who smoke are devalued as individuals and discredited as a member of society; they are stigmatized.
- Results: We caution about some important negative consequences arising from the stigmatisation of smokers. (note: paper gives several examples)
- Full Study on Sci-Hub
- Few low SES smokers questioned their smoking status, instead framing smoking as a ‘fact of life’. However, there was also a clear sense that tobacco control, and its adherents, are contributing to a sense of stigmatised identity for these smokers.
- Stigma is a mark of social disgrace that arises within social interaction (Goffman, 1963). It disqualifies bearers of the mark from full social acceptance.
- The results suggest that British smokers are identified via a negative aesthetic marker, consisting of smell and appearance. Like all stigmatized marking, they are not assessed merely at a cognitive level, but emotionally too (Jones et al., 1984). Non-smokers report repulsion, dislike, irritation, sickness and, most often, disgust in the face of them.
- Full Study on Sci-Hub
Articles, Websites, Blogs - Smoking/Nicotine (Stigma)
- “The political climate and the concerns of the anti-tobacco and anti-smoking advocacy groups has made it harder to do this kind of research,” he explained. “It has impacted our ability to recruit people to our studies.”
- Instead of stigma, we need an open and unfettered discussion.
- Public health campaigns that stigmatize smoking can backfire, according to a study published Monday, leading some people to become so angry and defensive that they refuse to quit and others feeling so bad about themselves that they give up trying.
- Smokers reported feeling shame, guilt and embarrassment for their smoking behavior and used words such as “leper,” “outcast,” “bad person,” “low-life” and “pathetic” to describe themselves, the study found. These feelings increased after failed attempts to quit smoking.
Studies, Papers, Reports, Articles, Blogs, Videos, etc. - Stigma, Smoking, and Lung Cancer
- "Unlike risk-based lung cancer screening focused exclusively on tobacco smoking, universal breast and colorectal cancer programs have simplified access and increased participation.28 Risk-specific guidelines may deter participation by implying lifestyle blame or creating eligibility confusion, compounded by stigma."
2025: Article: The hidden reason lung cancer screening is not working
- By: Lisa Carter-Bawa, Ph.D., M.P.H., N.P.
2025: IASLC Podcast: “Please Don’t Tell My Family”: Stigma and Lung Cancer
- Featuring: Narjust Florez MD - Lisa Carter-Bawa PhD, MPH, APRN - Jamie L. Studts PhD
2023: Article: Stigmatization of smoking-related diseases is a barrier to care, and the problem may be on the rise
- "The study, conducted by a team of researchers led by Nathan Harrison, a behavioral scientist and Ph.D. student from Flinders University, in Australia, aimed to identify and synthesize existing interventions to combat stigma associated with lung cancer and smoking-related respiratory diseases, including chronic obstructive pulmonary disease (COPD)."
- By: Skip Murray
- Patients expressed clear preferences for CCPS to refrain from using judgmental labels when assessing smoking history, including a preference for questions such as “have you smoked cigarettes in the past 30 days” rather than “are you a smoker?” . This perspective is consistent with the broader clinical efforts and dissemination of resources to reduce illness-related stigma through the increased use of person-first language and other bias-free language in clinical care and research. [emphasis added]
- One in four (25%) people in the UK agreed that they have less sympathy for people with lung cancer than other forms of cancer. Globally, one in five (21%) people agreed that they have less sympathy for people with lung cancer than other forms of cancer.
- "Attention to the robust causal connection between smoking and lung cancer, although crucial for tobacco control, may have unintended consequences that generate blaming responses and biased negative perceptions toward patients with lung cancer..."
- By: Narjust Florez, MD, FASCO
2017: Decreasing Smoking but Increasing Stigma? Anti-tobacco Campaigns, Public Health, and Cancer Care
- "Public health researchers, mental health clinicians, philosophers, and medical ethicists have questioned whether the public health benefits of large-scale anti-tobacco campaigns are justified in light of the potential for exacerbating stigma toward patients diagnosed with lung cancer. Although there is strong evidence for the public health benefits of anti-tobacco campaigns, there is a growing appreciation for the need to better attend to the unintended consequence of lung cancer stigma. We argue that there is an ethical burden for creators of public health campaigns to consider lung cancer stigma in the development and dissemination of hard-hitting anti-tobacco campaigns. We also contend that health care professionals have an ethical responsibility to try to mitigate stigmatizing messages of public health campaigns with empathic patient-clinician communication during clinical encounters."
- "Findings support an association between lung cancer stigma and delayed medical help-seeking behavior. Therefore, lung cancer stigma is a potential barrier to timely medical help-seeking behavior in lung cancer symptoms, which can have important patient outcome implications."
- Regardless of smoking status, lung cancer patients have reported stigmatization from clinicians, family members and friends due to strong associations between smoking and lung disease.
- The results of this study confirm our previous findings that LCS [lung cancer stigma] is positively correlated with anxiety and depression and negatively correlated with QOL [quality of life].
- "There is qualitative evidence that from the patients’ perspectives public health programs contribute to stigma about lung cancer and this was supported by published commentary."
Studies, Papers, Reports - Employment and/or Insurance (People Who Use Nicotine)
- "In the present study, 400 Canadian and US hiring professionals evaluated a candidate’s resume and then cybervetted their social media page which disclosed their gender and smoking status (i.e., cigarette smoker, vaper, or nonsmoker). Revised evaluations post-cybervetting were lower for applicants discovered as smokers and vapers than for nonsmokers, but vapers were perceived as negatively as smokers."
- “Tobacco users tend to have lower incomes, which is often a barrier to coverage,” Barber said. “Charging them more to access the care they need … is harmful and inequitable. The VPHA is cautiously optimistic that this barrier will go away, and people will be able to afford quality coverage and get the care they need for their tobacco use and beyond.”
2020: Occupying multiple stigmatized identities: Smoking and unemployment stigmas among the unemployed
- Study findings support the need to examine stigma – in particular, multiply occupied stigmas – as an important social determinant of health. Stigma may relate to job-seekers’ employment opportunities, efforts to quit smoking, and physical and mental health. Greater attention to multiply occupied stigmas and experimental investigations to identify novel strategies to reduce stigma are warranted.
- In addition to the health and financial harms associated with smoking, the “smoker” label today may also carry stigma
- The association of smoking and unemployment stigmas with depressive symptoms is consistent with prior findings of an association between lung cancer stigma and the severity of depressive symptoms
- Our review found that some smokers experience self-stigma such as self-loathing and shame as a result of public stigma. The few studies on structural interventions suggest that they affect some smokers in counterproductive ways, such as eliciting defiance and/or prompting public and self-stigma.
- Importantly, no studies examine stigma-related impact of newer structural interventions, such as higher insurance premiums or worksite policies to employ only nonsmokers.
- To advance the field, it will be critical to pinpoint whether, when, and how denormalization becomes stigmatization. [emphasis added]
- Removing the stigmatizing aspects of existing approaches, and creating new interventions that avoid stigmatizing smokers, may help further enhance the reach and effectiveness of tobacco control.
- Sci-Hub (full paper)
- The very fact that the Affordable Care Act moved away from health status-based rating in the individual market, with conspicious exceptions for tobacco use and wellness program participation, is telling. The ACA then suffers from an internal tension. On one hand, its supporters framed it as “a civil rights bill for the sick.” On the other, despite eliminating health insurance practices that explicitly disadvantage people based on health, the ACA permits — even encourages — health insurers to charge more to people who use tobacco. Pursuant to the tobacco surcharge, an insurer can opt to charge a tobacco user up to fifty percent more for the same health plan. While many health insurance companies may not opt to charge the full penalty, the ones that do could price out smokers and other tobacco users.
- It then comes as no real surprise that the Affordable Care Act’s tobacco surcharge may actually backfire, leading people to drop health insurance rather than to quit smoking. Given both the intervention’s ineffectiveness and its lack of a clear justification for regulating tobacco use and no other health status, we propose that singling out tobacco users may be the result of animus.
- The tobacco surcharge singles out smokers and other tobacco users, thus communicating
- (1) that tobacco use has social meaning as a category,
- (2) that using tobacco is socially undesirable,
- (3) that classifying people based on their tobacco use is acceptable, and
- (4) that tobacco users should face disadvantage in the form of a heightened premiums.
- In other words, the tobacco surcharge mirrors the process of stigmatization. Thus, even if the tobacco surcharge is not driven by animus against smokers, the ACA could lay the foundation for stigmatizing tobacco users.
- Smokers face similar kinds of regulation outside health insurance. Some employers refuse to hire nicotine users of any kind. As one set of authors explain, workplace bans, “by sanctioning discrimination, abrogate smoker’s rights as ‘ordinary citizens’ by placing ‘them’ in a category that separates smokers from ‘us’(non-smokers).
- What emerged from this review is current anti-smoking campaigns are not effective for smokers who are living in poverty. These findings suggest that anti-smoking campaigns need to limit stigma and build programs that are effective for all socio-economic classes.
- Anti-smoking campaigns have been used for the last three decades, and while there has been a decrease in smokers across the US, the number of smokers living in poverty has remained relatively unchanged. The research points to the use of stigma as a possible reason for smokers who are living in poverty to not stop smoking. The use of stigma to help a population, who may be stigmatized for multiple reasons, has shown through the research, to be a poor tool in moving them towards a smoke free life. The use of stigma in public health campaigns may lead to making things worse for smokers who live in poverty through discrimination in hiring policies and other unintended consequences.
- Smokers had a lower likelihood of reemployment at 1 year and were paid significantly less than nonsmokers when reemployed.
- While there is evidence that internalizing smoking stigma may prompt some individuals to quit smoking, this review also suggests that smoking self-stigma can have profoundly negative consequences for some smokers and may make quitting more difficult.
- Currently, there may be an overreliance on strategies which focus on negative reinforcement including both strategies to change smoking norms and increase smoke-free public spaces as well as more structurally stigmatizing policies such as basing hiring decisions and health insurance costs on smoking status.
- Many health care organizations, such as the Cleveland Clinic and Baylor Health Care System, and some large non–health care employers, including Scotts Miracle-Gro, Union Pacific Railroad, and Alaska Airlines, now have a policy of not hiring smokers — a practice opposed by 65% of Americans, according to a 2012 poll by Harris International. We agree with those polled, believing that categorically refusing to hire smokers is unethical: it results in a failure to care for people, places an additional burden on already-disadvantaged populations, and preempts interventions that more effectively promote smoking cessation.
- Structural forms of discrimination perpetrated against smokers and former smokers (e.g., company policies against hiring smokers) are also related to smoker-related stigma.
Articles, Websites, Blogs - Employment and/or Insurance (People Who Use Nicotine)
- "How do most life insurance companies define 'smoker'? Usually, life insurance companies use very specific questions to find out whether you are a smoker or not. "The insurance companies consider an individual as a smoker if they take nicotine in any form like bidi, cigarettes, cigars, hookahs, chew tobacco, etc," says Pankaj Goenka, Assistant Vice-President & Head-B2B Business, Insurance Dekho. Even if you use a nicotine patch or gum, the insurer can classify you as a smoker."
- At the turn of the year, U-Haul announced that starting in February, they will “decline job applicants who are nicotine users” in the 21 states* where it’s legal to do so. And it doesn’t matter if the nicotine comes from a cigarette, a patch, gum or a vape.
- More bad news for smokers and vapers: The city of Dayton, Ohio, says it will no longer hire anyone who uses nicotine or tobacco.
- " These new policies essentially treat cigarettes like illegal narcotics. Applications now explicitly warn of “tobacco-free hiring,” job seekers must submit to urine tests for nicotine, and new employees caught smoking face termination."
- "Federal laws allow nicotine-free hiring because they don't recognize smokers as a protected class. There’s no data on how many U.S. businesses won't hire smokers, but the trend appears strongest with hospitals."
- "These policies engender controversy, and we recognize that they risk creating or perpetuating injustices. One set of concerns arises from the fact that tobacco use is more concentrated in groups with lower socioeconomic status. Hospitals do better than most institutions at creating employment and advancement opportunities for disadvantaged populations. So even though most members of lower socioeconomic groups do not use tobacco, and even though anti-tobacco hiring policies are not intended to reduce jobs for these populations, they are likely to do so inadvertently, at least somewhat."
- Smokers now face another risk from their habit: it could cost them a shot at a job.
- "Smokers will no longer be eligible for employment at the World Health Organization, the agency has announced. Effective immediately, all job applicants will be asked if they smoke, and if so, whether they are willing to quit. The application process will be terminated in the case of smokers who refuse to stop."
- "The rule will extend to users of chewing or snuff tobacco."
"Relapse"
- Suggested words to use instead of relapse(d): recurrence (appears to be the most widely used), return, resume (resumption), slip, lapse, (use) episode, substance use (no strings attached to current, former, daily, random), revert, recent use... these and other suggestions can be found on this question posed on Twitter in the comments.
Articles, Websites, Blogs - Relapse
- Much of society associates the term “relapse” with failure because of an antiquated and baseless condemnation of individuals with substance use disorder who do not become “cured” with their first treatment. Very often, there is immediate judgment.
- I propose that if we want to help erase stigma, we choose to use the word recurrence rather than relapse. “Recurrence of substance use disorder” creates a more accurate connotation, one that is more consistent in the medical world.
- Our language activates implicit cognitive scripts that give meaning to what we try to convey and communicate.
Use of Stigma/Shame to Prevent Initiation or to Encourage Cessation
- Information about the campaign from the late 80's and early 90's. (Using language like "stupid," "silly," and "butts.")
- Tweet with photo of animals smoking poster.
- "Some educators were wary about “whether the materials were appropriate for use in the schools."
Lessons Learned: Substances, Alcohol, Incarceration, Illnesses, Disabilities, Mental Health, Weight, etc.
Studies, Papers, Reports - Language/Stigma
- "The purpose of this study was to determine the rate and frequency of labeling language, emotional language, and person-first language (PFL) toward individuals with substance use disorders and addictions in articles published in 24 counseling journals. Of the 249 articles reviewed, 61.04% did not fully adhere to PFL, while 34.54% included labeling language and 51.41% included emotional language. A significant positive correlation was found between the use of labeling language and emotional language. Implications for practicing counselors, counselor educators, and researchers are provided. We advocate for the use of PFL toward those with addictions in published works and in conversations."
- "Stigma, defined as societal labeling and mistreatment based on perceived differences (Link and Phelan, 2001) leads to a divisive “us” versus “them” dynamic that leads to status loss in a context of power dynamics. Substance use stigma (SUS) involves negative stereotypes and discrimination toward people that use substances, which results in limiting their access to needed resources and impeding wellbeing (Livingston et al., 2012). Stigma is pervasive in society and based out of moral judgments that substance use is bad or wrong (Room, 2005)."
- "SUS significantly hinders treatment and education, adding to the burden carried by people with substance use disorders (Keyes et al., 2010, Kulesza et al., 2013). It limits access to treatment through underfunding of substance use treatment services (Saloner et al., 2014, Zemore et al., 2021, Calabrese et al., 2016, Luoma, 2010) and creates barriers to reintegrating into communities (Neale et al., 2011)."
- Shaping a more effective response to obesity can start with the careful use of language that frames obesity in ways that are person centered, scientifically accurate, easily understood, and limits risk of bias.
- "The majority of patients with substance-related diagnoses had at least one note containing SL. There were also several patient characteristic disparities associated with patients having SL in their notes. The work suggests that more clinician interventions about use of SL are needed."
- Coalition for Diversity and Inclusion in Scholarly Communications
- In most cases it is preferable to emphasize the person over the attribute. For example, “person with cancer” instead of “cancer patient”, “man in prison” instead of “inmate.” Emphasizing the attribute can reduce the person to a label and dehumanize them.
- The results of a separate manual search (n = 110) on the Wiley Online Database showed that approximately 30% of articles used the term "alcoholic" in a stigmatizing manner.
- Stigmatizing language can perpetuate negative biases against people with alcohol use disorder. We encourage researchers to shift away from language that maintains discriminatory conceptions of alcohol use disorder. Reducing stigma has the potential to increase rates of treatment seeking and improve treatment outcomes for individuals with alcohol use disorder.
2021: Choosing appropriate language to reduce the stigma around mental illness and substance use disorders
- "The words we use to describe mental illnesses and substance use disorders (addiction to alcohol and other legal and illegal drugs) can impact the likelihood that people will seek help and the quality of the help they receive. Research indicates that stigma—negative attitudes toward people based on distinguishing characteristics—contributes in multiple ways to poorer health outcomes; consequently, it has been identified as a critical focus for research and interventions"
- "Stigma is particularly difficult to eliminate, even with educational and other interventions, and carefully considered language is only one part of addressing it. But it is also one of the most immediate ways in which researchers and others who communicate about stigmatized conditions can effect change."
- This guide is intended to raise questions about language and commonly used phrases and terms, with the goal of cultivating awareness about dominant narratives and offering equity-based, equity-explicit, and person-first alternatives.
- In these simple examples, we can start to recognize the power of language to frame our thinking; equity-focused, person-first language seeks to center the lived experience of people and communities without reinforcing labels, objectification, stigmatization and marginalization.
- This guide is not intended to be a definitive and all-encompassing instruction manual. Instead, it was written (with humility) to stimulate heightened awareness and dialogue. We offer this guide as a tool, knowing that efforts to nurture change in contentious spaces requires courage and commitment. Undermining systemic oppression and the dominant narratives that sustain them will not happen by chance. Reclaiming and promoting a social justice narrative will require intentional and collective action.
- "Weight bias and stigma exist in a variety of realms in our society (media, education, employment, and health care), and unfortunately many view it as a socially acceptable form of discrimination. Patients with obesity often avoid scheduling appointments for health promotion visits and routine care due to perceived weight bias and stigma from their health care provider."
2021: Media framing of emergency departments: a call to action for nurses and other health care providers
- "Two overarching themes were found. First, in ED-related media that portrays health care needs of people experiencing health and social inequities, messaging frequently perpetuates stigmatizing discourses..."
- Substance use stigma is prevalent throughout the health system and contributes to poorer quality of care and negative health outcomes.
- Creating a stigma-free health system will require collaborative action and sustained commitment of key players across the health system.
- Efforts to reduce substance use stigma within the health system must also acknowledge and address intersecting stigmas, including through initiatives not traditionally labelled as “anti-stigma interventions”.
- Shame-induced stigma most damages those already vulnerable, reinforcing health disparities.
- Global health use of shaming tactics can inadvertently worsen health-damaging stigma, especially for those with the least power.
- These effects, that drive additional health disparities and suffering, are difficult to prevent.
- Ethically and practically, stigma should never be deployed as a global health tool because the effects are often both unavoidable and invisible to outsiders.
- Words matter. Certain words can make people or groups feel excluded, and can also convey stereotypes, expectations or limitations based on a person’s identity...
- Language changes. As societal values change over time, so does the language that is considered acceptable...
- Mindset matters. Be open and empathetic, and encourage others to do the same...
- Person first. Use ‘person first’ language: language that prioritizes someone’s identity and individuality above whatever other characteristic you might be describing...
- Be inclusive. Try and use language that is as inclusive as possible to reflect the known or unknown diversity of your audience. For example, instead of using the terms husband or wife when unsure of the sexual orientation and/or marital status of who you are speaking with, use the term ‘partner.’ Similarly, when referring to a group of people, try ‘folks’ instead of ‘guys.’
- Be specific. Use language that is consistent with how a person identifies and is comfortable for them...
- Be critical. Before introducing or describing someone based on personal characteristics (such as race, gender identity, (dis)ability, use of substances, etc.), ask yourself whether it is relevant and necessary to do so...
- Results provide further evidence that previously identified stigmatizing labels have the potential to influence medical care and medical practitioner perceptions of individuals with substance use disorders and should be avoided.
- As highlighted in the Publication Manual of the American Psychological Association, many labels can be perceived as pejorative and stigmatizing.
- We can continue to model stigmatizing and pejorative language that politicians and the media will no doubt take one step further, or we can start changing the way we talk about the men, women and young people we work with and research, in the hope that they too will change.
- "We consider the role language plays in the SUD treatment field and how the language and concepts the words convey keep individuals from growing through and past the SUD. We argue that a new understanding calls for a shift in language among providers of SUD care in which the culture of SUD treatment begins to emphasize 'thriving' rather than 'recovery' from SUDs."
2018: Substance use, recovery, and linguistics: The impact of word choice on explicit and implicit bias
- The general public, treatment professionals, and healthcare professionals have been found to exhibit an explicit negative bias towards substance use and individuals with a substance use disorder (SUD).
- Results support calls to cease use of the terms "addict", "alcoholic", "opioid addict", and "substance abuser". Additionally, it is suggested that "recurrence of use" and "pharmacotherapy" be used for their overall positive benefits. Both "medication-assisted recovery" and "long-term recovery" are positive terms and can be used when applicable without promoting stigma.
- Weight stigma is often propagated and tolerated in society because of beliefs that stigma and shame will motivate people to lose weight. However, rather than motivating positive change, this stigma contributes to behaviors such as binge eating, social isolation, avoidance of health care services, decreased physical activity, and increased weight gain, which worsen obesity and create additional barriers to healthy behavior change. Furthermore, experiences of weight stigma also dramatically impair quality of life, especially for youth.
- Our results verify that just by placing the word “person” as the first one in the label we use, we can, at least partially, avoid the stigma induced when “epileptic” – as being the main determinant of that certain person – is used.
2014: Pejorative Language
- Some words can hurt. Slurs, insults, and swears can be highly offensive and derogatory.
- This article champions the use of person-first language as a foundation for recovery-oriented practice and enhanced collaborative treatment environments that foster respect, human dignity, and hope.
- "The use of labels is one way stigma is perpetuated by eliciting the label's stereotyped narratives onto an individual or group. Within harm reduction discourse, the word "addict" can have detrimental effects on how the public perceives people experiencing addiction and their deservingness of pragmatic services. This article aims to draw attention to the inattention we give "addict" in language and explain how its routine use in society acts to perpetuate addiction stigma. Using the example of supervised injection site opposition in Canada, the use of "addict" is used as a way to understand how stigma through language works to impede the expansion of harm reduction initiatives."
Articles, Websites, Blogs - Language/Stigma
- Identifying a condition as ‘stigmatising’ can show us how living with this condition can lead to negative social experiences such as discrimination, judgement, social exclusion, vilification, ostracism, labelling, loss of status, prejudice, unfair treatment, among others.
- It is important to understand shame because it is shame that drives behaviour and decision-making, and in healthcare contexts, shame can easily lead to disengagement, non-disclosure, lying, withdrawal and avoidance.
- Research has shown that reducing stigma makes it more likely that affected substance users will enter and maintain treatment.
- “Abuse” is an ugly word. “Child abuse,” “sexual abuse,” “physical abuse,” “emotional abuse,” “domestic abuse.” And then, of course, there’s “substance abuse.”But one of those things is not like the others: In all of the other types of abuse, there is a perpetrator who is harming a victim.
- "Harm reduction at its core is a strategy against stigma. Giving people the space and freedom to manage their own health without judgment or coercion is a core component. Harm reduction is not just a strategy to minimize the risks of drug use, but a philosophy for self-care and community care that promotes compassion, openness and practical knowledge that can improve and save lives."
2021: People First Charter
- The People First Charter launched in July 2021, during the Berlin International AIDS Society Conference, to promote person first HIV & Sexual Health language.
- Language matters. People living with or at risk of HIV experience stigma & discrimination and the wrong language perpetuates this.
- One study found that the terms “addict” and “substance abuser” led people to hold distinctly negative associations about the people they described. Another found that replacing less obviously pernicious terms, like “relapse” and “medication-assisted treatment,” with “recurrence of use” and “pharmacotherapy,” resulted in more positive views of people with substance use disorders.
- While centering research design around what matters most to people with sleep disorders is critical, research communication must be similarly people-centered. One approach is using “people-centered language” in both professional and public communications. People-centered language is rooted in sociolinguistic research demonstrating that language both reflects and shapes attitudes. People-centered language puts people first, is precise and neutral, and respects autonomy.
- Sleep researchers may worry that adopting people-centered language will be onerous or hinder the use of elegant shorthand. However, convenience should not take priority over reducing stigma and better engaging the people this research is intended to serve.
- "The new edition of its widely used AP Stylebook declares that "addict" should no longer be used as a noun. "Instead," it says, "choose phrasing like he was addicted, people with heroin addiction or he used drugs." In short, separate the person from the disease."
- "The new language has been widely welcomed. "It's very good — really well done," says John Kelly, an associate professor of psychiatry at Harvard and founder and director of the Recovery Research Institute at the Massachusetts General Hospital. Kelly was the lead author of a study published in 2010 that showed that clinicians — from the least educated up through doctoral-level professionals — take a more punitive stance when patients are described as "substance abusers" rather than "people with substance use disorder."
- Originally published on Undark
- "These labels erased my humanity. Total strangers felt allowed to criticize or judge me, saying that I was ‘such a waste of life,’ ‘useless,’ or ‘just a drunk or addict.’ These words also carried the connotation that I was lazy, selfish, or a criminal. After a while, I began to believe these words, concluding that I no longer served a purpose, had opportunities, or deserved hope."
- There are several kinds of stigma that cause negative attitudes, stereotypes, shame, and fear toward people with addiction.
- When we are not called mad dogs, animals, predators, offenders and other derogatory terms, we are referred to as inmates, convicts, prisoners and felons — all terms devoid of humanness which identify us as “things” rather than as people.
- In an effort to assist our transition from prison to our communities as responsible citizens and to create a more positive human image of ourselves, we are asking everyone to stop using these negative terms and to simply refer to us as PEOPLE. People currently or formerly incarcerated, PEOPLE on parole, PEOPLE recently released from prison, PEOPLE in prison, PEOPLE with criminal convictions, but PEOPLE.
- Links to several documents
- The OAC has identified many areas where weight bias penetrates today’s society, such as media, entertainment, healthcare, employment, education and more. However, one of the most prevalent areas that the OAC is now tackling to eradicate weight bias and stigma is language. The OAC, along with other obesity-focused organizations in the community, are raising awareness of a new initiative titled People-First Language.
- What Does Stigma Look Like?
- Stigma limits a person’s ability to access services they need because they feel unworthy of receiving or requesting services.
- Stigma creates barriers while receiving services by people feeling unwelcome or judged by program staff that offers services.
- "The foundation of most societal issues is rooted in hierarchies and ideologies. These two concepts are bound together by one term: stigma. Stigmas support hierarchies and give power to ideologies. Each level of any hierarchy is bound to be linked to a stigma, whether the stigma is about the people, their attitudes, mannerisms, professions, or other factors. Though often compared to their cousin, the stereotype, stigmas have much darker undertones."
- Using people-first language - Language matters in compassionate care, especially in behavioral health care, and that doesn’t mean just what you say in front of a patient. What you say behind closed doors with coworkers can be the seed for stigma and perpetuate discrimination against a person based on a physical or mental disorder. Using people-first language means speaking in a way that primarily acknowledges the person, rather than the illness or disability. Thanks to Linden Oaks Behavioral Health for being a source of this poster.
Social Media
2022: Dr. Anna Maria Valdez
- Twitter thread about hurtful ways to deal with someone trying to educate others about stigmatizing language and best practices for when being made aware of such language.
Opposing Views - Smoker or Person-First
- Twitter thread
- Response: Overlooked Inequities in Language May Undermine Progress in Tobacco Control: Further Thoughts on the Need for Reflection
- Original: Time to Stop Using the Word “Smoker”: Reflecting on the Role of Language in Advancing the Field of Nicotine and Tobacco Research
- "Ultimately, the key is to ask, whenever possible, how a person chooses to identify, rather than making assumptions or imposing your own beliefs. Each person’s relationship to language and identity are deeply personal, and everyone’s identity choices are worthy of respect. I, who proudly chooses identity-first language and identifies as a disabled woman, am worthy of respect. Being who you choose to be – who you are – is something no language rule should ever take away."
2017: Editorial Perspective: The use of person-first language in scholarly writing may accentuate stigma
Roadblocks and Barriers to Using Person-First Language
Suggestions to add to this page
- “Advancing Health Equity: A Guide to Language, Narrative and Concepts (including person-first language)
- Central to our discussion is the research literature concerned with the concept of state-paternalism in tobacco control—the line between an ethically justified interference with the freedom of those who smoke and an exaggerated infringement disproportionate to the same people’s right to live as they choose.
- In countries with an already advanced infrastructure for tobacco control, this dilemma might become quite intrusive for regulators. We ask that if people, who smoke are aware of and have accepted the risks, are willing to pay the price, smoke exclusively in designated areas, and make decisions uninfluenced by persuasive messages from manufacturers—is a further tightening of anti-smoking measures still legitimate?
- Conclusion: We recommend that a further intensification of smoking control in countries that already have a well-developed policy in this area requires that regulators start to exploit the opportunity that lies in the ongoing diversification of the recreational nicotine market.
- Karl Erik Lund and Gunnar Saebo; Harm Reduction Journal (2024) 21:33https://doi.org/10.1186/s12954-024-00951-w
- Funding: Norwegian Institute of Public Health (Governmental)
- Ontology - Stigmatizing labels. The difference between addiction and dependence.